(Full outline is available through Archives Canada)
SECTION 5 CNA YEARS
SECTION 5.1 -PILOT PROJECT FOR EVALUATION OF SCHOOLS OF NURSING
5.1.1 Appointment as Director of Pilot Project for Evaluation of Schools of Nursing in Canada -Leave of absence for 2 years from VGH
5.1.2 Arrival in Ottawa (44 lbs. baggage) -stay at Bytown Inn
5.1.3 Initial Planning -Meeting with Special Committee of Project in Toronto and Montreal -Selection of Schools for Pilot Project -Selection of Regional Visitors -Appointment of Liaison Committee -Publicity for project -Familiarization trip across Canada -Meeting with Minister/Deputy Minister of Health and/or Education & Chief Nursing Officer -meeting with directors of schools to be surveyed and administrative personnel of hospital/university -meeting with nurses organizations in the community
5.1.4 Survey of 25 schools of nursing in all to provinces (Fr. & Eng.) -Personnel in schools -data provided -survey techniques -unusual incidents -interim meeting with executive committee (Board of Directors)
5.1.5 Writing of report in Ottawa and Maple Ridge
5.1.6 Presentation of Final Report to Executive Committee (B of Dir) 1959-60 -4 months Teachers College in New York -presentations to annual meetings
5.1.7 Halifax June 1960. ”Elle a gagné ses épaulettes” -acceptance of 4 recommendations
5.1.8 Personal approaches to fill other special positions (see 5.2) -Director of Special Studies 1960-63
(return to Teachers College in New York to complete doctorate)
SECTION 5.2 DIRECTOR OF SPECIAL STUDIES -CNA
5.2.1 Appointment as Director of Special Studies (condition of appointment -extension of VGH Leave of Absence)
5.2.2 Development of Plan to Implement 3 of 4 recommendations of Pilot Project -Directors of project recruited -Rec. 1 Kasper Naegle -study of whole field of nursing education. -Rec. 2 School Improvement Program (G. Rowsell) -Rec. 3 Evaluation of Quality of N.S. (L. Campion) -Supervision of Special studies: Rec. 1, 2 and 3 -Assistance with writing and publication
SECTION 5.3 ROYAL COMMISSION
5.3.1 Death of Kasper Naegle. CNA Project (Rec. 1) and RCHS project on Nursing Education combined
5.3.2 RCHS Project Director -defined purpose of project -planned survey of university schools of nursing and diploma schools of nursing -on-site visit to university schools of nursing 16 basic (p.75) -?? Personal -recommendations
SECTION 5.4 EXECUTIVE DIRECTOR – CNA
5.4.1 History of CNA
5.4.2 Appointment as Executive Director
5.4.3 Special Projects (Library, Statistics)
5.4.5 International initiatives -ICN (CNR) – speaker and chair sp. Sessions Frankfurt, Montreal, Mexico, Tokyo, Nairobi, Los Angeles, Tel Aviv, Seoul, Madrid -Red Cross -WHO (U of Edinburgh) -Lebanon -Commonwealth Caribbean (Reg.Nsg.Body) -Government Delegations -Middle & Latin America -Summit Seminars -Caracas, Venezuela -Commonwealth Nurses Fed. (1971) -Montevideo, Uruguay -Expansion of International Programs (CIDA) -30th WHO Assembly -World Federation of Public Health
In the 1990s, Helen Mussallem worked closely with Elizabeth Crawley to record Helen’s personal stories in an autobiography. They intended to address all of Dr. Mussallem’s life, from her childhood in Maple Ridge to her retirement years.
Only parts of sections 5, “The CNA Years,” and section 6.1.4., “Commonwealth Nurses Federation”, were written. The original outline(click to view) reveals their intentions for the autobiography project. The text went through several handwritten and typewritten drafts, with corrections and revisions by Helen Mussallem and Elizabeth Crawley. This website version of their work contains all of their completed text, arranged in chronological order.
In 1960, when Helen Mussallem wrote the preface to Spotlight on Nursing Education: The Report of the Pilot Project for the Evaluation of Schools of Nursing in Canada, she noted that only factual information was presented in the report and that “…someday the other part of the story may be written.” Someday is here. Helen’s adventures and experiences, during this exciting and critical professional journey, provide a unique, fascinating glimpse into the turbulent world of nursing education in the 1950s.
Does Canada need a national program of accreditation for diploma schools of nursing? When this question was first asked, decades ago, at a CNA biennial meeting, Helen Mussallem was serving with the armed services (WWII) and such matters had never crossed her mind. Indeed, in her early years of nursing practice, she was convinced that such subjects were best left to the “old maids” in the profession. Resolutions “approving the principle of accreditation” were passed almost biennially until 1955 when a significant step was taken. Nursing leaders of the day looked with approval at the U.S. accreditation system and believed that such a program would have a great positive impact on Canadian schools of nursing.
Accreditation was the main theme at the 1955 CNA General Meeting. Helen remembers it well: a hot, stuffy room for approximately 150 delegates –air conditioning was a luxury in those days! The opening session, although well planned, ran into some minor obstacles. When the minister did not arrive to deliver the opening prayer, some kind soul found a prayer in her purse and gave it to the president to read. Unfortunately, also during the session, the president, G. Sharpe, lost her front tooth and the organist lost the music for the opening to God Save the Queen. CNA was one of the first professional health organizations to provide translation services to its members but this also proved hazardous as so many people tripped over the electrical connections laid across the floor that they had to be disconnected.
Discussion on accreditation raged on. Helen was sitting in a pool of perspiration when she heard the president ask Miss Mussallem for her opinion. She remembers somehow getting to the microphone and saying that there should be an accreditation program as soon as possible. How profound! As director of Canada’s then largest school of nursing, she was sure a more scholarly statement had been anticipated.
For Helen, life at the Vancouver General Hospital School of Nursing continued as busy and exciting as ever until, unexpectedly, Trenna Hunter, president of CNA and fellow resident of Vancouver, asked her to become Director of the Pilot Project. No hesitation here! Helen’s response was a quick and positive … “No!” although she would be willing to serve as a Regional Visitor. “No” was her only possible answer because both her parents had serious health problems and because she had become inextricably linked with her young niece, Lynette, who taught her the meaning of “unconditional love”. Professionally, she enjoyed her work at VGH School of Nursing and had implemented some exciting and innovative curriculum changes. Why leave all of this for two years?
As time passed, Helen began to feel considerable pressure to accept this assignment and, reluctantly, a positive answer emerged. “Yes.” Little did she know how much that response would change the whole course of her life.
Arrival in Ottawa (5.1.2)
It was agreed that Helen would begin her work on the Pilot Project for Evaluation of Schools of Nursing in September 1957. As her first working day was to be the day after Labour Day, she arrived at Uplands Airport in Ottawa on Sunday and was whisked away to her home away from home, the Bytown Inn. As she travelled through the city, she couldn’t believe her eyes and thought she had been transported back to the Middle Ages. There were old street cars rumbling all over, everything looked old and dingy. The Bytown Inn was an old wooden structure and her room was on the ground floor. The only view to be had was of a gas station and her nose was constantly assaulted by fumes from the garage. If it had been possible to return home then and there, she would have been ecstatic! The next day, she begged to have her room changed and, finally, one was found for her on the second floor. When she had looked around, she asked curiously what the rope was for and was told that, in case of fire, she was to use the rope to slide down to the ground floor! To add to her welcome to Canada’s capital, a staff member from CNA called later to say that she had forgotten to meet her plane. What a feeling of gloom and doom!
Initial Planning of Pilot Project for the Evaluation of Schools of Nursing (5.1.3)
Helen was tense meeting the staff at CNA’s office at 270 Laurier Avenue. The four senior staff were gracious and kind but, oh, the loneliness of it all! The next day she was off to Toronto and Montreal to meet members of the Special Committee for the Project, all well known and respected Canadian nurses. They were all so clever and knowledgeable that she was almost paralyzed talking with them. She remembers wearing the “proper” suit bought for the Project: navy blue with detachable collar and cuffs, the latter to be washed and pressed each night –no wash and wear in those days. Also, as so few women travelled in the 50s, attaché cases were great, heavy ones made for men. She was justifiably proud of her genuine leather, hand-crafted briefcase but it weighed so much, even empty that she suffered from a sore arm for ages.
What was CNA Headquarters like? Friendly … after at time. But Helen had grown up in a different professional milieu. Since she was from B.C. – a leader in Canada in the Union movement of professionals — she was thought to be painted pink or red, or at the very least to be a Union sympathizer. The word “union” was unacceptable in the professions but all knew that the last meeting Helen had attended as an RNABC Board Member was held to decide if the nurses in one of the inland hospitals should go on strike when the hospital would not honour the decision of the government arbitrator. Helen remembers discussing the situation until 3 AM, until it was decided that nurses would withdraw their services in all but essential areas. This was a first for nurses in Canada. She remembers leaving the meeting in downtown Vancouver, in the early morning hours, so exhausted that she walked straight into a puddle up to her ankles and felt nothing until she returned to her suite to find water and mud oozing from her boots.
Helen’s first months at CNA were hectically busy, but she did not mind as she had few social engagements in the evenings. Occasionally, she would sneak across the river to Hull for a change of milieu. What was on her plate as Director of the Pilot Project for Evaluation of Schools of Nursing?
– development of criteria for the evaluation of the schools
– preparation of preliminary information schedule
– role of National Office in the survey
– preparation of list of data required at the time of the survey
– preparation guide for the survey week
– preparation of a format for writing the report in both English and French
Most daunting of all, was the schedule prepared by National Office to: first, visit all officials in national and provincial health departments as well as a one-day visit to each of the 25 schools to acquaint them with the project and to show that Helen Mussallem did not have “two heads”. There was much anxiety across the country as this project was, incorrectly, viewed as an accreditation program; and, second, to prepare a cross schedule.
Travel in the ‘50s was more difficult than it is in the 90s and hotel accommodation in smaller communities left much to be desired. On the first series of one-day visits, there were many surprises. Helen remembers getting off the train in a small Ontario town in mid winter. Emerging from the train, there was only one taxi to be had so all four travellers squeezed in. Helen told the driver she would like to go to the “X” Arms Hotel. Silence. All other passengers left –one by one. When the driver began to drive into the outskirts of town, Helen became suspicious and asked if the “X” Arms was a good hotel. “Yes,” said the driver. When he stopped, a startled Helen saw, through the dark night, a two-story, run-down building with a huge dog out front. Again she asked if this was a good hotel and again the driver replied in the affirmative. The Project Director will never forget the scene that greeted her as she walked into the hotel: a densely smoke-filled room with drunken men chasing women around the room. She was asked to sign an ancient book and then was pointed to her room. Unbelievable! Panel in door ripped off, etc. She recalled her orientation at the Nursing League for Nursing and their advice that, in such a situation, one should go to the phone and call another hotel. She ventured into the main room again only to be told there was no phone in the hotel and that the nearest phone was two blocks away. Nothing to do, but to place the half clean towel over the bedspread, covered with dog hairs, and lie down. What a night! Women screaming and men running up and down the halls ALL night. She stayed fully clothed on the bed and, as dawn broke, splashed water on her face, paid for her room, and set out on foot to find the nearest phone. A gas station about two blocks away permitted her to phone “the best hotel” in “X”; a cab was dispatched and she arrived at a lovely, modern hotel and made for the dining room. All white linen, flowers and well dressed people. Life was real again. Across the dining room, Helen spotted a VON nurse she had met in Ottawa. When she told her story, the nurse said” Wait a minute. A student of yours is a VON nurse here and I want you to tell her about last night.” Helen did. The former student opened her big, brown eyes and said, “Miss Mussallem, did you stay there ALL night?” “Yes,” Helen replied. “Tell me what kind of hotel is it?” “Well,” said the VON nurse, ”we hold a clinic there from time to time.” Enough said.
Then there was the time when Helen’s plane to St. John’s, Newfoundland arrived very late. Ten men and Miss Mussallem lined up at the Hotel Newfoundland for their rooms. Helen was at the end of the line as her luggage slowed her down ascending the stairs. There was great shouting at the front desk when the reception clerk announced that they would all have to share rooms. They all shrieked about “confirmed reservations” but there were no rooms to be had as there had been no flight out for departing guests. Almost as a person, they turned and looked at the lone female. Helen just stood there and waited only a few minutes. A porter came and whisked her to a lovely single room overlooking the harbour.
Those were also the days when, leaving an elevator, you made sure you had your keys in hand as there was usually someone following. Strange were those days when few females travelled on business. At another school of nursing, on a one-day visit, the director of the school arranged for a corn roast in the evening. All the teachers and local members of the professional association were present. Corn was passed around. Helen decided that, instead of presenting a speech, she would ask for questions. The audience sat quietly as someone asked a question, then as Helen paused before replying, all simultaneously chewed across a row of corn. What a sight –speaking to 20 cobs of corn! So, while the audience was formulating questions, Helen joined in the chewing of the corn.
The North Bay visit will always be remembered by the Director for the sleepless night spent at her hotel. A convention of salesmen had decided to spend the night on the main floor, drinking the hours away. Despite Helen’s frequent pleas to the management, it was 6 A.M. before the noise ceased. Although in no condition to conduct a proper orientation visit the next day, the Director did her best.
Having completed one-day visits to the 25 large, medium and small size schools of nursing, located in all provinces, the Director selected the various types of diploma programs to be surveyed –the three-year diploma hospital program, the two year plus one year internship program, and programs with close university affiliation. The goal of the survey, “To determine if Canadian schools of nursing are ready for a program of accreditation and if it is feasible at this time to initiate such a program”, seemed more daunting than ever.
The achievement of this goal was, of course, not the Director’s sole responsibility. There was, as always, a committee structure set up to assist the Pilot Project Director. This “democratic process” was meant to ensure that CNA members felt involved and would be able to claim some ownership of the finished product.
The first committee struck was the Special Committee which the Executive Committee of the CNA Board of Directors charged with initiating work on the project until a director was appointed. Although little preliminary work had been done when Helen arrived in September of 1959, the Executive Committee continued to Special Committee “…to advise the Director of the Pilot Project, upon her request, on matters of administration and policy”. Members of this committee were leaders in nursing education in Canada: Sister Denise Lefebvre, Rae Chittick, Sister Mary Felicitas, Margaret Street, Katherine MacLaggan, and six more. They were all eminently knowledgeable and well-recognized in the Canadian nursing community and they scared the new Director to death! Helen says, “Even though they treated me as a competent person, I’m not sure I was. I said many times that I may not be an expert in the field but I had a strong sense of commitment to achieving the goals of any work I undertook. This trait was acquired from my parents. We learned that we must work hard and only play after the job was done”.
The Special Committee soon determined that there was, and would continue to be, a need for interpretation of the project to allied professional agencies. Hence, a Liaison Committee was appointed. Members came from the Canadian Joint Committee on Nursing (equal representation from Canadian Medical Association (CMA), Canadian Hospital Association (CHA) and CNA, plus a representative from the Canadian Public Health Association, the Canadian Association for Adult Education and two members of the Special Committee on the Pilot Project. Meetings were infrequent and often held at CMA headquarters in Toronto. Helen remembers entering the CMA building by a side door and meeting in a room with inadequate heating and no air conditioning, which was considered a luxury in those days. She has a clear recollection of being “allowed in” the side door of CMA headquarters but, in 1962, when she had completed her doctorate, the front door suddenly swung open and, from that moment on, the Director was allowed to use the front door.
The times being what they were, it was difficult to assess how well this committee succeeded in interpreting such a “massive project on Canadian nursing education” to the seven national organizations.
The nature of the pilot project required that a qualified Board of Review study the survey reports, written by the Project Director, and pass judgment on the educational programs of the schools survey, i.e., using present criteria, if a program of national, voluntary accreditation were in place, would the school be accredited?
This was an incredibly hard-working committee. Each member of the Board of received a copy of each completed report as soon as it was duplicated at national office. They then studied the reports before the committee’s final meeting in May of 1959. To prevent any possible bias, schools were identified only by a code number.
Although not a committee, Regional Visitors were an integral part of the surveys. Following the National League for Nursing pattern, two regional visitor surveyors were selected for each school of nursing. This was intended to ensure that the report would provide a balanced judgment of each school. On each visit, the Director acted as senior visitor and the regional visitor as second visitor. For French-language schools of nursing, a third person –the senior bilingual visitor –played an integral role. She, with the assistance of a second bilingual visitor, was responsible for conducting surveys in the five French-language schools. The Director also participated on this team. Not only did she have overall administrative responsibility for surveys in these schools, but she translated the French language reports into English.
Little did Helen realize, when she agreed to be Director of the project, that she would be faced with such a formidable task of planning, organizing and directing the Pilot Project as well as coordinating all activities related to it. Her responsibilities included:
– Travelling to all 25 schools across the country on a preliminary visit; interpreting the Project to directors of the schools, and orienting them to the process of the survey;
– Conducting orientation workshops for regional visitors and an orientation program for the Board of Review;
– Taking overall responsibility for the surveys of the schools by:
– organizing each field survey trip;
– writing the survey report with the regional visitor
– validating, clarifying and supplementing information;
– setting up an organizational structure;
– providing guidance to schools within the field of her competence; and
– interpreting the project to hospital personnel;
– Establishing all procedures and organizing meetings of the Special and Liaison Committees;
– Interpreting the purpose and scope of the Project to deputy ministers of health, education, allied professional groups and the general public, via press, radio and television media.
How the new Director gained the skills necessary to conduct such a massive survey is a story in and of itself. As CNA had decided that a Canadian nurse should direct this Project, after one short week in Ottawa, Montreal and Toronto, Helen was sent to National League for Nursing headquarters in New York to become a competent surveyor. The time allotted for this training was four months!
This intense orientation program was invaluable to the fledgling Director’s future work. To make the indoctrination to the accreditation process as thorough as possible, no effort was spared by National League for Nursing staff. Helen was asked to serve as one of two accreditation visitors on six full-fledged accreditation visits in various geographical areas in the United States. Each of
these six surveys was carried out with a different National League for Nursing visitor to enable the new Canadian Director to study variations in survey techniques as well as the personal, philosophical variations of National League for Nursing staff. Surprisingly, Helen’s problems as a National League for Nursing visitor were unrelated to her expertise. She had a Canadian accent! Should the school being surveyed learn that one of the visitors was a Canadian and if perchance, the school did not receive accreditation, the whole process might have been condemned. Helen was continually reminded to say “OWT” and “ABOWT”, etc. and, luckily, as she had obtained her master’s degree at Teachers College, Columbia University, she was aware of the required accents. Frequently, the staff of the schools surveyed asked where she came from and Helen always replied “the Pacific Northwest” which was true as Vancouver was home. At each school, she always asked, immediately, some personal question like, “Where did you receive your basic education?” or “Have you always lived here?” She had quickly learned that most people are always happy to talk about themselves. Only once did she find herself being grilled and, thankfully, the senior National League for Nursing visitor saw her predicament and called on her for advice. Whew! She had another tense moment when some nurses in Duluth, Minn. took the National League for Nursing visitors for a drive and wanted to take them across the Canadian border. What to do? It would be a bit hard to explain Helen’s Canadian passport! Some miles from the border, the senior visitor again came to the rescue by advising that they really didn’t have time for such a long drive. Saved again!
The novice Director soon became accustomed to the pressures involved in conducting a survey. Each survey was one week in duration: five and a half days were spent on the survey with the remaining time being allocated for travel to the next school to be visited. One full day and evening (Monday) was spent at the hotel studying all written materials describing the program. Three days (Tuesday, Wednesday, and Thursday) they were at the school, visiting and each night and all day Friday was spent writing the report. Helen vowed, there and then, that she would develop a tool to assist in writing the reports as she found that, by ten or eleven P.M., their minds were so numb that they could hardly think of one decent descriptive noun or even the correct verb. Eventually, her “tool”, used in Canada, was so successful that it was adopted, with revisions, by her National League for Nursing mentors. The report was read to the school and hospital staff on Saturday morning, with opportunity allowed for correction of errors. The completed report was shipped to National League for Nursing headquarters and then it was on to the next survey. At National League for Nursing, after six surveys, the visitors took one week off. This luxury was not possible in Canada as staff was very limited and the entire project was conducted over such a short period.
Helen’s first stop as an National League for Nursing visitor was in the hot, humid Delaware city well known for being the Dupont headquarters. She recalls leaving Delaware on a stiflingly hot day and standing on the platform waiting for the train to her next post. The platform was level with the train entrance but, as she entered the train carrying bags in both hands, her shoe got wedged between the station platform and the train. Not knowing what else to do, she stepped on board, dropped her bags, and then turned to retrieve her shoe. Unfortunately, the train had started and her shoe was swept away. So, there she was, sitting in the back seat, one shoe on and one shoe off contemplating how to get a pair of shoes out of her luggage. The train stopped at the next station but the aisles were full so, off the train and into Penn station she limped –an unusual sight in 1957, but no one stopped or even stared. In the Ladies Room, she retrieved another pair of shoes from her suitcase and discarded the lone shoe in a wastebasket.
Each town –like DuPont in Delaware –seemed to have some special claim to fame. When Helen was posted to Little Falls, Minn., she was sure there would be nothing there. In fact, she even had difficulty finding it on the map. Imagine her surprise when she met with the faculty, and guess what? They proudly pointed out that Little Falls was the birthplace of Charles Lindbergh!
On Helen’s return to New York, work at National League for Nursing headquarters was intense. She formed many warm, rewarding relationships with National League for Nursing staff during stressful times spent preparing for the Board of Review and reporting to committees, etc. When it was time to return to Canada in early January 1958, she was sad. After such warm camaraderie at National League for Nursing, she was again on her own.
The new Director’s orientation was complete. The next step: the long awaited survey of 25 Canadian schools of nursing.
1.1.1. Mussallem Family
– historical & current
Grandparents
Parents (SM escape from Lebanon)
Siblings (p.136)
Relatives – Mussallem & Bassette
1.1.2 Prince Rupert – the beginning (SM p.75)
-sidewalks – stores – reading – church – S.S.Prince George – carried on board
-Ocean Falls
-Howe Sound
1.1.3 Vancouver
-Why Vancouver? – SM “could not abandon country of his childrens’ birth”
-SM’s training in motor repairs
apprenticeship years
-soap enterprise (86)
1.1.4 Maple Ridge and Port Haney
– Establishing home
-Establishing Haney garge
-Began school
-Church, sporting, organizations, public library, post office (federal)
-SM in municipal politics (107)
Reeve/mayor for 22 years
-A.M. and the Queen (115)
-Pre-school activities
-School – Haney Public School
SECTION 5.1 -PILOT PROJECT FOR EVALUATION OF SCHOOLS OF NURSING
5.1.1 Appointment as Director of Pilot Project for Evaluation of Schools of Nursing in Canada
-Leave of absence for 2 years from VGH
5.1.2 Arrival in Ottawa (44 lbs. baggage)
-stay at Bytown Inn
5.1.3 Initial Planning -Meeting with Special Committee of Project in Toronto and Montreal
-Selection of Schools for Pilot Project -Selection of Regional Visitors
-Appointment of Liaison Committee -Publicity for project
-Familiarization trip across Canada
-Meeting with Minister/Deputy Minister of Health and/or Education & Chief Nursing Officer
-meeting with directors of schools to be surveyed and administrative personnel of hospital/university
-meeting with nurses organizations in the community
5.1.4 Survey of 25 schools of nursing in all to provinces (Fr. & Eng.)
-Personnel in schools
-data provided
-survey techniques
-unusual incidents
-interim meeting with executive committee (Board of Directors)
5.1.5 Writing of report in Ottawa and Maple Ridge
5.1.6 Presentation of Final Report to Executive Committee (B of Dir) 1959-60
-4 months Teachers College in New York
-presentations to annual meetings
5.1.7 Halifax June 1960. ”Elle a gagné ses épaulettes”
-acceptance of 4 recommendations
5.1.8 Personal approaches to fill other special positions (see 5.2)
-Director of Special Studies 1960-63
(return to Teachers College in New York to complete doctorate)
SECTION 5.2 DIRECTOR OF SPECIAL STUDIES -CNA
5.2.1 Appointment as Director of Special Studies (condition of appointment
-extension of VGH Leave of Absence)
5.2.2 Development of Plan to Implement 3 of 4 recommendations of Pilot Project
-Directors of project recruited
-Rec. 1 Kasper Naegle -study of whole field of nursing education.
-Rec. 2 School Improvement Program (G. Rowsell)
-Rec. 3 Evaluation of Quality of N.S. (L. Campion)
-Supervision of Special studies: Rec. 1, 2 and 3
-Assistance with writing and publication
SECTION 5.3 ROYAL COMMISSION
5.3.1 Death of Kasper Naegle. CNA Project (Rec. 1) and RCHS project on Nursing Education combined
5.3.2 RCHS Project Director
-defined purpose of project
-planned survey of university schools of nursing and diploma schools of nursing
-on-site visit to university schools of nursing 16 basic (p.75)
-?? Personal
-recommendations
SECTION 5.4 EXECUTIVE DIRECTOR – CNA
5.4.1 History of CNA
5.4.2 Appointment as Executive Director
5.4.3 Special Projects (Library, Statistics)
5.4.5 International initiatives -ICN (CNR) – speaker and chair sp. Sessions Frankfurt, Montreal, Mexico, Tokyo, Nairobi, Los Angeles, Tel Aviv, Seoul, Madrid
-Red Cross
-WHO (U of Edinburgh)
-Lebanon
-Commonwealth Caribbean (Reg.Nsg.Body)
-Government Delegations
-Middle & Latin America
-Summit Seminars
-Caracas, Venezuela
-Commonwealth Nurses Fed. (1971)
-Montevideo, Uruguay
-Expansion of International Programs (CIDA)
-30th WHO Assembly
-World Federation of Public Health
5.4.6 -Schools of Nsg. To Education system
-CNATS
-CNA House
-Status of Women
-Countdown
-ICN Congress ‘69
-Chain of Office
-CNF (1962)
-Research Unit
-Letters Patent
-Briefs & Position Statements
(Physicians’ Assistant)
-Brief Putting Health into Health Care
-Doctoral preparation for Nurses (Seminar)
-NWTRNA
-Expanded Role for Nurses
-Health Promotion Program
-Special Advisor to Cdn. Nurse delegation and offices at ICN meetings Geneva, Frankfurt, ??, Montreal, Dublin, Mexico City, Tokyo, Nairobi
5.4.6 Personal Etc. -Honors & Awards (OC)
-Social Life
SECTION 6 RETIREMENT AND BEYOND
6.1.1 Transfer of responsibilities to CNA & CNF to new Executive Director, Feb. 81 -Board of Directors
-staff
-allied health professionals
-records (social wants)
6.1.2 Consultant to new Executive Director -planning and problems
-clarifications
-relationship with staff
6.1.3 ICN – Election as member of Board of Directors (July 1981) -Board meetings in Geneva 81-85
6.1.4 Commonwealth Nurses Federation -Lectureship in West Africa – Nigeria, Ghana, Liberia, Sierre Leone, Malta and Cyprus
-Lectureship on PHC (“Continuing Education: an essential to nursing strategy and networks in primary health care”)
-Model lecture and special description in each country and WACN
-Relationships with governments and professional nurses associations
-Caribbean P.H. Association (founding member)
6.1.5 Other International Assignments -Project Hope – Virginia, USA – Keynote Speaker ‘81
-World Congress on P. Health Care – speaker ‘83
-Consultant and speaker Nursing & Health Cuba ‘81
-Official ICN Representative to second World Congress on Nursing
-Chair, Planning Session, World Federation of Public Health ‘87
-WACN/ECSN/PAHO
6.1.6 National commitments and participation -Economic Council of Canada (1971-1990)
-VON Board & President
-CPHA Int. Review & eval. Committee -1993
-Premiers Council on Health Strategy – 199?
-Human Rights Institute for Canada – Board of Directors, 1981 –
-St. John Ambulance – Chair Nsg. Advisory, Advisor to Chancellor, Nurse to Jerusalem Project
– CIDA (NGO Division)
-WHO
-Caribbean Regional Nursing Body
-Cdn. Society of Assoc. Executives
-CCSD
-Consultant to YM/YWCA Discussion Club
-Cdn. Lung Assoc./Cdn. Nurse Pers?
-USN
-CUSO
-Law Reform Commission
-Coalition of National Voluntary Organizations (& Board of Directors)
-Ont. Occ. Health Nurses Association (Cert. Ctee)
-H & W Canada – WHO fellowship selection ctee
-Canadian Cancer Society – Fellowship Cttee
-Friends of Rideau Hall – member
-Friends of Canadian Museum of Civilization
-National Gallery of Canada
-National Arts Centre
-CNF
6.1.7 Personal -social life
-courses taken
-awards
-special projects
-travel
Yes, and they wanted me to go to the combined course with the University of B.C. and the Vancouver General Hospital. But all my friends were going to the Vancouver General Hospital so I went there. What was this degree business? I wasn’t going to be bothered. They were a bit snobbish too, the degree people. So I went into Vancouver General Hospital, and then subsequently went on for my degree work, to McGill and what-not.
George Post: What are your strongest recollections about doing that RN course at Vancouver General?
Well, a lot of things. I think that could take an hour or more, at minimum. There were so many things that as a very young girl at 19, when we went in training, I had never seen anyone die. That was quite traumatic. We didn’t have counselling and so on like they have now. People coming into Emergency in Vancouver, the General took them all in. They were all badly dismembered or cut up or so on. And all these things were really, they’re still traumatic. But you know we were not told about, well, we were told there’d be accidents, and you did this to wounds, and so on, but there was no counselling. Like now, if somebody sees a terrible situation, they counsel them a bit. We somehow survived all that.
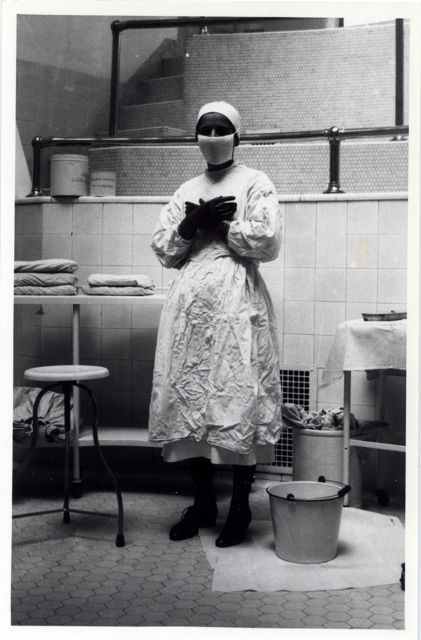
Helen dressed to go into the VGH Operating room.
But there were a number of things. I was just listening to the radio this morning, when you saw doctors doing things that were not ethical or not correct. And I remember at that time there was an anaesthetist that everybody said to watch him, we weren’t allowed in the room. And he would always put the mask on his face first, and have a little whiff of the gas. He was really hazardous, now I look back at it. But nobody reported him, people sort of closed ranks.
But there were a number of things when you are a student nurse, you see so many things. I had never seen anybody born of course; I fainted the first time. (laughing) I wouldn’t have except that the lady that supervised said, “If you are going to faint, faint quietly.” I just crumpled up against the wall.
There were all sorts of tales that one could tell about training, how we helped each other along. They used to have the Infectious Disease Ward… The Infectious Disease Ward was one thing, and of course I was a patient there because I got scarlet fever. But they had the Venereal Disease Wards for really very hush-hush… You see at that time they didn’t have the same medications, and they were all put down in rooms below ground at the Vancouver General. Well, they wanted to keep them out of sight I guess, for one thing, and secondly, I guess there was underneath it all there was sort of an ethic that they had ‘done wrong’ so we were going to put them in these beds. And a lot of gonorrhea with the women, I can remember that so well. And tuberculosis of course was quite prevalent in my training. And two of my classmates died of tuberculosis.
George Post: But they contacted you at the hospital?
Oh yes, yes, oh yes, at the hospital. And everybody had to take these man 2 tests and you could tell whether you were exposed to TB or not. And mine was never positive. Everybody else in the class except me. And I don’t know why, I guess it is the reaction. But tuberculosis was really a hazard. There were a number of hazards that students in training would have.
I have gotten off the track of what you were asking about.
We weren’t coddled but we were watched, and the people there, they had a really ‘way out’ idea that we should be educated rather than trained. Because in other hospitals even today, although it’s not the same system, they were using the students, they were indentured labour. But not at the Vancouver General. It was really well thought out, by and large. When I look back I couldn’t believe it because I didn’t know anything else, except that we thought we were better than St. Paul’s. But that was rivalry in the city.
George Post: Did you ever consider going to medical school rather than to nursing?
It never really appealed to me, I must say. I don’t know why. I think I was always in admiration of what doctors did, and working with the doctors was always a very positive experience. But I never thought of becoming a doctor. I never thought I was really clever enough, to be quite honest. I never thought I could do it. Because some of the courses and so on, at that time, required a pretty high intelligence. And I was, I have to admit, a rather shy, timid person in many ways, although I didn’t like to show it. And I just thought I just couldn’t do it. Maybe I could have, I don’t know. Whatever I did I have enjoyed it all and I have never looked back.
George Post: You told me that one of your sisters was also a nurse.
Yes, but after me. She was older than me and when I would come home with these great tales, she wanted to be a nurse then. And I said, “Oh Mary.” Yes, she did. “You sound like you were having a lot of fun.” “Oh,” I said, “it’s hard work too.” But she went in after me.
George Post: To the same hospital?
The same hospital, yes. But I had finished by the time she came in. She had some special permission, because you had to be 19 or 20. If you were 21 you were a bit old, I think she was probably 21, 22. Yes, we both graduated from the same hospital.
George Post: Now your brothers, who went on to school and university,y did that in Vancouver?
Yes, my both brothers went to UBC. My oldest brother didn’t, but they both went to UBC. It was, well, it was the only one; the next one would have been in Edmonton. There weren’t as many colleges or schools, no college system at that time, as we know it today. It was Normal School, but no Junior College system.
Mowat, ? , Helen Mussallem about to go their rounds for the V.O.N.
During the Director’s orientation in New York, a previously-prepared questionnaire was sent to the director of each participating school of nursing. The questionnaire had been adapted from the Application for Accreditation (diploma program of National League for Nursing) and its purpose was:
– to obtain as clear a picture as possible from the school of its educational program for those who would make the visit and those who would evaluate the program; and
– to assist the faculty in making a critical evaluation of its program.
Later, many schools indicated they had derived great value from completing the questionnaire and, if the Pilot Project had gone no further, they would have found this step a most helpful one in the evaluation of their school. This response was gratifying. Every one of the 25 questionnaires, with requested additional material, was returned to National Office by November 1957 –prior to the return to Canada of the Project Director.
The main portion of the preliminary phase of the Pilot Project, however, was the one-day visit to each school across Canada which participated in the Project. During this phase, it was deemed advisable that a one-week survey visit also be made to one school so that the necessary alterations to the evaluation process could be made prior to phase two –the survey of the remaining 24 schools of nursing.
This complete, one-week survey was to serve as a trial run. There was some concern that the detailed evaluation process might not be appropriate as this was an entirely new educational process in Canada. On completion of the trial survey, the Director was gratified to find that the process worked very well. In fact, only minor revisions were necessary. She remembers that, when they read the report of the first one-week survey to members of the school of nursing and senior hospital staff, they were amazed. Their school was considered to be one of the best and most innovative in Canada and they had anticipated a glowing report. The regional visitors had written in as objective a manner as possible and the summary contained a listing of “Areas of Strength” and “Areas Requiring Study and Improvement”. The director of the school, who was also a member of the Special Committee, was appalled at the number of weaknesses listed but none were challenged. Helen found the process to be extremely uncomfortable. This, the first school to be surveyed, was located in one of Canada’s largest cities and their living facilities, therefore, were better than those found in many of the smaller centers. The second regional visitor for this survey was a religious sister. As there was a bar in the dining room, Helen was so embarrassed at the thought of Sister looking at a bar, that she always seated herself facing it. On completion of the survey, during dinner, Helen suggested to Sister that this was a time for celebration. Much to the Director’s surprise, Sister recommended they have a sherry and, being so relieved to have the first survey over, they even managed a second one with a brandy to finish off the evening. Helen was very glad that she had packed her bags for early morning departure before dinner as she could just barely make it to her room. In those days, as a result of her “Presbyterian upbringing”, she had rarely consumed alcohol.
The four-month preliminary phase of the Pilot Project concluded with an interim report to the CNA General Meeting in Ottawa where the Director also chaired a panel presentation “Guidelines for the Future”. The continuing task of keeping CNA membership informed throughout all phases of the project was still a priority. Press releases were prepared, articles were published in The Canadian Nurse and memoranda were sent regularly to executive secretaries/directors of each provincial association, the Special Committee, the Executive Committee and selected governmental and non-governmental agencies.
The intermediate phase was spent primarily in completing the survey of the remaining 24 schools of nursing across Canada. In the Preface to The Report of the Pilot Project, Helen wrote, “… items that should be recorded when travelling ‘from Cape Race to Nootka Sound’. There was ample opportunity for the unusual to happen…” And happen it did. Then she went on to say, “The modes of travel and accommodation were many and did not lack variety.” When the survey was finally completed, over 57,551 miles had been travelled and cross country interviews had been conducted with 1,759 people, exclusive of contacts at meetings of nurses and allied professional groups. Additionally, there were numerous contacts with press, radio and television media.
The one-week, comprehensive survey of the 25 nursing schools was as varied as the size and the geographic location of the school; the control; the type of program –three year diploma, two year plus one year’s internship, programs with a university affiliation, and even a diploma course within a psychiatric hospital. Also taken into consideration was the ratio between anglophone and francophone schools. At the time of the Pilot Project for Evaluation of Schools of Nursing, there were 174 diploma schools of nursing in Canada. Selection of the schools to be surveyed was made using scientific sampling techniques which were later validated by nationally-recognized researchers.
The data obtained from the schools surveyed during the Pilot Project is carefully documented in Spotlight on Nursing Education: The Report of the Pilot Project for the Evaluation of Schools of Nursing in Canada. As stated in the preface of that publication, “Someday the other part of the story may be written.” This is the “other part” of that unique and fascinating story.
1957 Prince Edward Island
My first trip to Prince Edward Island was fascinating. As we approached the Island, I could see great stretches of red earth from my plane window. It seemed to cover a huge part of that little province island. I also noted, with pleasure, the long stretches of sandy beach but, as it was early spring, I was not consumed with the idea of going swimming.
On landing, the ANPEI President and Executive Secretary met me at the foot of the airplane steps. They welcomed me most hospitably and insisted on driving me around Charlottetown, by car, before checking me into my hotel. I was worried, unnecessarily, that my hotel reservation would be cancelled if I arrived too late. Little did I know then that, on the Island, “everyone knew everyone else.” Many of them were, in fact, related through families which had lived in PEl for many generations.
As we drove along, my companions were not impressed by my enthusiasm for the red earth. It is, apparently, iron-saturated clay which sticks to one’s car and anything else with which it comes in contact. Our first stop was the historic Parliament Buildings. As we approached the front steps, my companions greeted, by his first name, a tall, distinguished gentleman -Premier Matheson. What a rare experience for me to meet the Premier of a province minutes after my arrival! After greeting the Premier, I was given a tour of the Parliament Buildings and the historic chambers where the debate, which led to Confederation, was held. A Commissionaire had been charged with showing us all the details of the Chambers. Despite being well informed, the rum on his breath was sufficient to intoxicate a bystander. Reverently, we read the well-known inscription, “Providence being their guide they builded better than they knew”. Our guide then insisted I sit in the chair once occupied by a Father of Confederation. So many times I have seen the picture of the gathering of the “fathers” after the signing, but the photograph really came to life for me as I viewed the windows always seen in the background. We drove along the beautiful coast to Cavendish to see the home of Anne of Green Gables. This was 1957, years before the marketing of Anne and the emphasis on tourism. The Islanders, although cautious of publicity, were aware of the need to keep the economy viable.
“Let Us Pray”
During the PPESN years, it was customary to have a prayer before each CNA meeting. Sometimes, the Lord’s Prayer was recited and, at other times, one of the religious sisters or a CNA officer led another prayer. I was rather sorry when this practice ceased as it gave all of us a quiet respite before the furore started. It was also an excellent way of calling a meeting to order.
When Sheila Nixon, Regional Visitor, and I had completed writing the report of the survey of a large, well-recognized school in a large metropolitan city, we discovered that the school was not nearly as well organized as we had thought. Nor did the school have the quality of education one would expect. It was, in short, a poor program. On Saturday morning, as was the schedule for all surveys, the completed report was to be read before the entire faculty and others in the school who wished to attend. One of the main reasons for reading the report was to allow those involved with the educational program to correct any misunderstandings that had been written into the report.
The Director of the school was very apprehensive so I decided to wait a few moments, until everyone was settled, before proceeding. While we waited, Sheila, not knowing the microphone was on, said, in a loud voice, “I think it is time for a good prayer”. I was not amused, nor was the school’s director. After hearing the report, I’m sure she thought the Sheila’s remark had been planned.
“The Owen Sound Incident”
During a school of nursing survey, the views of students regarding their educational program were not overlooked. They made a significant contribution by describing to us various aspects of their program. Usually, our conference with the students was scheduled for one hour but, frequently, it continued much longer. The group of students, selected by the president of the students association, was usually comprised of officers of the student organization together with students from each class in the school. Members of the faculty were requested not to attend this discussion so that it might be informal, with as free an exchange of ideas as possible. As the students discussed, informally, various aspects of their courses, it was possible to identify the real philosophy of the school and the degree to which the program was planned for, and with, the students. It also opened up new visions of what the students perceived as their role as graduate nurses in the whole health care system.
The faculty usually accepted our reasons for wishing to speak with the students alone, although some were more gracious than others. At one school in central Ontario, I had just begun the discussion with students when I had a tickle in my throat. I signalled to the Regional Visitor to carry on and, not wanting to disturb the group, tiptoed quietly to the door to get a drink of water outside the room. When I opened the door -lo and behold -there was the Director of the school, a very tall lady, bending down with her ear to the keyhole, trying to catch every word. Never have I seen a more startled look on the face of a Director. I quietly excused myself and carried on down the hall. She didn’t follow or ask if I needed assistance. I was embarrassed for her and, as there was no way of rectifying her action, I never mentioned it again. I must confess, however, that this incident tainted the remainder of the survey for me because neither of us was at ease with the other.
“Wash My Horses”
The survey of the school of nursing in Rimouski, Quebec was unique for me as it was my first experience in a completely francophone environment. I hadn’t appreciated that this city and its hospital and school of nursing was so isolated from Anglophone Canada. When we met with the students, not one spoke English fluently. These were all bright young girls in their late teens but they seemed completely unaware of any major events in the rest of Canada. The students urged one of their number to speak with me in English — and she really tried. All the other students were consumed with gales of giggles at her efforts as her English was almost unintelligible. I found out later that this was not unusual in French Canada of that period. The opposite was, of course, also true in Canada’s Western provinces and in most parts of Ontario.
On these surveys, I was very fortunate to have Sister Denise Lefebvre as senior bilingual evaluator and another Francophone sister who acted as Regional Visitor. I was responsible for the overall survey arrangements and translated the French-language report into English for the Board of Review. I attended all of the French-language interviews but, wisely, did not interfere with Sister Lefebvre’s comments, etc.
As sometimes happened in the Gaspe, there were difficulties with transportation and we were forced to stay in Rimouski until Sunday. I told Sister that I was going out to make a hair appointment for Saturday. When I returned triumphantly with an appointment for 11:30 a.m. the next day, I proudly explained how capable I felt, having negotiated all the arrangements in French. Sister doubled over with laughter. Apparently, I had asked to have my horses (chevaux) washed and set instead of “mes cheveux”. My French communication skills were very limited in those pre-CNA days.
Based on the National League for Nursing model, we always insisted on staying at hotels rather than accepting hospitality from the hospital or school of nursing we were evaluating. This, we believed, would ensure that the survey visitors would not feel indebted to the hospital which might color the objectivity of the report.
In one town in Nova Scotia, however, there was no suitable hotel — in fact, no real hotel at all. This was a preliminary visit and I was alone so I was housed on the private ward of the hospital. After several sessions with senior administrators, faculty, etc., I had dinner and returned to my room on the private ward. While reading my notes, I saw a young student pass my door and look in –but she said nothing. A few minutes later, she walked by again, rather slowly. When she went by a third time, appearing to hesitate in front of my half-opened door, I went to the door and greeted her. She immediately asked, “Would you please help me?” “Of course,” I replied. She explained, rather timidly, that the patient in the room next to mine looked rather strange and would I please come and have a look. I could tell immediately that the man was dead –very dead. I instructed her to call her supervisor while I remained with “the patient” until she returned. “Oh, no,” she quivered, “I’m afraid of the supervisor. She will be very angry with me.” When I told her that she had no alternative, she started crying but, again, I insisted that she call the supervisor RIGHT AWAY. With tears streaming down her face, she reluctantly left the room to call. I remained until I heard the supervisor approaching and then left the dead patient’s room via the bathroom we shared in common.
This incident raised many questions for me. Why had a student, in her sixth month of training, been left in charge, on the evening shift? Why was the young student able to communicate with me, a stranger, but afraid to call her supervisor? How could one ever condone such a situation — first from the patient’s perspective and, secondly, was this “nursing education”?
“Sterile Glasses”
When we were conducting the survey of the Glace Bay, N.S. school, we resided at the “Island Hotel”. It was touted by John Fisher, “Mr. Canada,” as the only hotel in Canada at that time to hang pictures of Canada on its walls. It was a comfortable hotel with the best sanitary features –especially in the bathrooms – sterilized drinking glasses, toilet seats, etc. I had always wondered how all this sterilization took place but I was soon to find out.
As my plane had been delayed, the hotel had allowed me to remain in my room until flight time. As I was resting in the room, the maid came in and started cleaning the bathroom. After exchanging a few pleasantries, she enquired, “Would you like to see how we fix our sterile glasses?” Of course I would. So, with my own eyes, I saw how she ran the glasses under very hot tap water, wiped them dry with my used bath towel and put on the “Sterilized Glass” paper cover. Likewise, the toilet was sterilized. I was appalled. Should I apprise the management of this practice — but I didn’t. In retrospect, I’d rather I didn’t know what might go on in any hotel purporting to have “sterilized bathrooms”.
Writing of the report in Ottawa and Maple Ridge (5.1.5)
The final phase of the pilot project included a detailed evaluation by the CNA Board of Review and the writing of the report for the entire project. In retrospect, it boggles the mind that the final report was ever written. It was so hot that long-ago summer in Ottawa –no air conditioning –that Helen was permitted to go home to B.C. to write. So it was in the spacious recreation room of her mother and father’s home in Maple Ridge that the landmark report was written. Helen wrote every day and almost every night. After breakfast with her parents, she took the reports of the 25 schools, minutes of meetings, correspondence, etc. from under her bed and went downstairs to write. She kept these priceless documents under the bed because, in case of fire during the night, she could rescue all the survey data. No photocopiers in those days!
Because of the nature of the report and the many tables she had developed, the Director worked with pen and pencil and a manual typewriter. As each section was completed, she toyed with the idea of mailing it back to National Office but was intimidated by the dilemma of writing new material in a descriptive report without being able to refer to previous chapters.
Helen remembers well, during the intensive writing process, hearing her father say to her mother, “I think Helen has taken on too big a job.” Her mother replied, “Don’t worry. She’ll get it finished.”
Each report –the record of joint observations and study by two visitors to each English-language school and three visitors to each French-language school–averaged 13,000 words and included approximately 14 tables for each school. Helen had little help in determining the format to be used in compiling this massive amount of raw data. Flashes of inspiration were essential and assistance from family members with a scientific background was a great value.
When the rough draft was completed, the long hours of fascinating work and the tight deadlines had all been worthwhile. The completed report was then typed, duplicated and sent, with much trepidation, to the Board of Review well in advance of their scheduled May 1959 meeting.
Presentation of Final Report to Executive Committee and Board of Directors (5.1.6)
1959-1960
When Board members met in Ottawa to discuss the report, they compiled a list, for each school, indicating areas of strength and areas requiring study and improvement. They also decided, on the basis of criteria used, which of the schools surveyed would have met the requirements for full accreditation, had such a program existed at that time. The voting of the Board of Review was believed to be significant in determining whether or not Canadian schools of nursing were ready for an accreditation program. It was recognized that the criteria used to evaluate the schools were not formulated by Canadian nurses. Following evaluation of the 25 schools, Board members were asked if they considered the criteria used to be applicable to diploma schools of nursing in Canada. There was consensus that, generally speaking, these criteria were applicable.
To review the survey reports, Board members used the criteria as a basis for judgment in evaluating each part of the program, using as a guide the booklet prepared for this procedure. This booklet, as well as all other materials and the survey report, was divided into the following sections of the educational program:
1. General Information on the School and the Controlling Hospital
2. Philosophy and Objectives of the School
3. Organizational and Administrative Aspects of the School
4. Instructional Personnel
5. Student Personnel Services
6. Curriculum
7. Evaluation of the Program and the Student
8. Library
9. Setting for the Educational Program
10. Records, Reports and Announcements
Under each section in the booklet were the statements of criteria used for evaluating each school. After studying the written report, each statement was considered and each member indicated whether or not this criterion was met by the school. If the data were not clear, this was indicated and an explanation was later provided by the senior visitor (the Project Director).
To provide as clear and detailed a picture as possible of the decisions of the Board, the data were presented in table form. These data indicated the total of number of schools, as well as the number of schools according to size, which met the criteria.
Although all members of the Board of Review did not vote the same way on each criterion, a very large percentage agreed of whether or not each criterion was met. When a member did not vote due to the fact, for instance, that she was a member of the school staff being visited, a record was made only of the number of Board members voting. In all cases, a substantial majority was required before a criterion was considered to have been met or not met.
In June 1960, the entire report was presented to the CNA Board of Directors and the report, and recommendations were presented to the annual general meeting of the Canadian Nurses Association held in Halifax.
Helen recalls, so vividly, the day in February 1960 when she presented her report to the formidable Board of Directors. When she had completed her presentation, she sat down with a sigh of relief. Unbelievably, the cold, calculating, critical members of the Board rose to their feet, as one, and gave her a standing ovation! Never, in anyone’s memory, had that Board given a standing ovation to anyone. Indeed, they rarely clapped or hardly cracked a smile, no matter what the issue. The President gave the Project Director such a moving tribute that the tears dripped down onto Helen’s clenched hands. Nurses of that generation never cried but, after the project’s long, convoluted journey, emotions just took over.
A four-month hiatus had been planned between the presentation of the report to the Board of Directors and presentation to the General Meeting in June. There was no money to pay the Director for this period. Helen decided to return to Teachers College, Columbia University, where she had earned her Master’s degree. A new semester was starting when she arrived, so she made an appointment to see her adviser, Dr. Anderson. Dr. Anderson had heard about Helen’s Canadian triumph and told her, then and there, that she was to earn a doctorate. One never said “No” to Dr. Anderson, but Helen thought she would do only one semester’s work until the CNA meeting in June. Dr. Anderson, however, knew she had gotten through to Helen and continued to goad her on.
Halifax June 1960 (5.1.7)
In June, the Director returned to Canada –first to Ottawa to touch base with CNA and then to Halifax to present her report to the membership. Sister Lefebvre, the Chair of the Special Committee, gave the first presentation and called Helen “Miss Accreditation”. Replying in kind, the Director addressed Sister as “Mother Accreditation” –that was ~ acceptable. When Helen had laid bare all of the findings of the national two-year study and had pounded home the recommendations, the entire body of French-speaking delegates rose, en mass, and sang “Ellea gagne ses epaulettes, malleuron malleurette….” Not to be outdone, the English-speaking group rose and sang “For she’s a jolly good fellow….” What a glorious ending –or was it the ending –of an exciting professional journey!
That biennial meeting in Halifax will always stand out in Helen’s memories. The report was not only accepted enthusiastically by CNA members but the media made it into a national event. CBC Halifax carried interviews with the Director on its newscasts and relatives and friends in Vancouver were able to view and listen. She had car and driver at her disposal and enjoyed the VIP treatment which came from all sides. While staying at the Admiral Beatty Hotel, where service was generally excellent, Helen remembers calling room service to order breakfast. To her request, room service replied, “Popper rice?” Mystified, the Director repeated, “I wanted to order my breakfast”. The operator repeated, patiently, “Popper rice?” Helen tried again –same response –and finally gave up. At breakfast the next day, she discovered that room service was asking if she wanted pop or ice!
Now the study was completed, the report presented to membership at the 1960 Biennial meeting, and three of the four recommendations were approved by the Executive Committee at their post convention meeting. I was asked to stay on CNA staff for one more year to implement the three recommendations of the Pilot Project.
I advised the Executive of my plans to return to Teachers College to complete my doctorate. I knew my financial resources were very slim but I was determined to complete the remainder of the two year doctoral study. They agreed that I should return to Teachers College for one semester and, when needed, fly to CNA for meetings to implement the three projects. This I did.
The amount paid for those days at CNA assisted greatly in buying books and food. My return trip to Teachers College was made with the now president Helen Carpenter, also a student at Teachers College.
The 1960 biennial meeting was over and an exhilarated Helen started on her return to Teachers College for the fall semester. She decided that the two Helens should go by bus to see the Acadian country and visit her relatives in Yarmouth. On their arrival, however, Helen Carpenter developed a serious chest condition and her uncle, a physician, ordered her to stay in bed. The doctor, a delightful gentleman of 91 years, was still practicing medicine and administering anaesthetics too. He told Helen Mussallem that he still used chloroform by the drip method. She was duly impressed –and amazed. Helen stayed with the Carpenters for an extra day but, as her friend was not improving, decided to try and figure out a way to get from Yarmouth to New York in time for registration and classes. She took the ferry to Portland Maine, getting incredibly seasick on the voyage, and eventually, via bus and train, made it to Whittier Hall in New York.
Whittier Hall was strictly a women’s residence, but Helen chose to live there so she would not be distracted by the many social activities at International House, and besides, she was closer to the library. Studying at the doctoral level was going to be a full-time job –especially as Dr. Anderson had mapped out a plan “to get her through” as quickly as possible. Helen was aware of her many commitments in Canada. She had completed one semester and was now returning for the second. She would then return to Canada for one year to collect data for her dissertation and carry out her new responsibilities as Director of Special Studies tor CNA, including implementation of three of the four recommendations of the Pilot Project.
Development of Plan to Implement 3 of 4 recommendations of Pilot Project (5.2.2)
On her return to Canada, project directors were recruited. Dr. Kaspar Naegle was engaged as Project Director for;
– Recommendation 1: “That a re-examination and study of the whole field of nursing education be undertaken”.
– Recommendation 2: “That a school improvement program be initiated to assist schools in upgrading their educational programs.”
Helen recruited Glenna Rowsell, already on CNA staff. Lillian Campion was persuaded to assume the position of Project Director to implement
– Recommendation 3: “That a program be established for evaluating the quality of nursing service in areas where students in schools of nursing receive their clinical experience”. As Director of Special Studies, Helen was responsible for the overall supervision of these projects.
– Recommendation 4: “That a program of accreditation for schools of nursing be developed by the Canadian Nurses Association” was held in abeyance pending completion of the other three projects.
Royal Commission on Health Services (5.3)
CNA Project and RCHS project on Nursing Education combined (5.3.1)
At this time, there was also general concern about the whole health care system. In 1961, a Royal Commission on Health Services was established with Justice Emmett Hall as Chair. It was the Commission’s intention to include an examination of the whole field of nursing and nursing education. It seemed logical, therefore, that Recommendation 1 on the whole field of nursing education be assumed by the person carrying out the examination for the Royal Commission. Dr. Naegle was a superb sociologist and scholar and Helen was delighted that he would be directing the project on nursing education for both CNA and the RCHS.
Royal Commission on Health Services Project Director (5.3.2)
The study for the Royal Commission on Health Services in Canada was an exciting and rewarding experience for Helen. The territory was familiar, but greatly expanded, from the report of the Pilot Project. It included not only diploma schools of nursing but university schools, nursing assistant programs, psychiatric nurse programs, operating room technician programs and midwifery courses. She especially enjoyed the field work which required many trips across Canada and her working relationship with researchers and RCHS staff, to whom she was responsible. Helen had been seconded to the RCHS by CNA from the summer of 1962 to May of 1963. The final report was published in 1964.
During the summer of 1962, CNA received a grant from Kellogg to create a Foundation and award fellowships. Applications were received from students and immediate awards needed to be made or the money for the current year would be lost. Katherine McLaggan, the prime mover in obtaining the grant, was responsible for forming a Selections Committee and, as it was August and no one else was readily available to meet with a committee, Helen was recruited.
She met with Katherine in her room at the Chateau Laurier in Ottawa where all the student applicant files were piled on the bed. While they were developing selection criteria for the awards, Helen was called to the Daly Building to meet with the Director of Research for the Royal Commission on Health Services and sign the contract for her study. While there, she met Mr. B. Blishen, Director of Research and Dr. Malcolm Taylor, Research Consultant. Dr. Taylor wished to speak with her at length and seemed slightly annoyed when Helen told him of her other responsibilities with Katherine McLaggan. When she related her encounter with Dr. Taylor to Katherine, she was told to phone him immediately and invite him to dinner. As he was already booked for dinner, Helen invited him to the Jasper Lounge for cocktails, where Katherine McLaggan used the encounter to great advantage, immersing him in the grave problems of nursing education. Helen’s role was to see that drinks were served without question and to be discreet about paying the bill. This being the pre-credit card era, she gave the waiter a $10 bill –ample for drinks in those days. She instructed the waiter carefully to serve as many drinks as requested. He did –but only one each –and, before Helen could get up to retrieve her change, minus tip, he brought the change to their table and plunked it down in front of her.
Helen was so embarrassed and Dr. Taylor was not amused. In those days, men always looked after the bill. After the drinks fiasco and dinner, Helen and Katherine went for a walk through the quiet Ottawa streets. Helen asked if Katherine had ever seen the face of the nurse at the back of the War Memorial. She hadn’t, so they scrunched around to get a better view. Just as Helen was pushing Katherine up the monument for a better look, the loud voice of a policeman shouted, “You ladies get down immediately or I will turn you in!” They both slid down ignominiously and vanished into the night. Up to the time she died, Katherine would recall this incident with great glee. During this period, and on into the 70s, Helen received many offers to assume the deanship of a university school of nursing or to become director of nursing at several large hospitals. She found only one offer tempting –to be director of the School of Nursing at the University of British Columbia. Even though CNA was planning to host the 1969 International Council of Nurses Congress in Montreal, Helen was assured CNA would wait for her. Negotiations continued.
As the School of Nursing had been on the UBC campus since 1916 and as two other health science faculties had been created at the university, the faculties of medicine and pharmacy, one of Helen’s requirements, an important one, was that the UBC School of Nursing also become a faculty. The negotiator sadly advised her that no change could be made as there already were too many faculties on campus. Finally, he arrived with what he termed “good news”. The Board of Governors had agreed that if Helen returned to UBC, the School of Nursing would become a faculty. Helen was delighted and asked to have the promise in writing.
This was impossible as the Board of Governors did not write such letters relating to the hiring of faculty! So Helen never accepted the UBC position and often wonders, if she had, what a different life she might have led. But that’s skipping way ahead of 1962. Let’s back up.
George Post: And you decided then to move right in to the University?
We had a choice, they called them Veteran’s Points. You could have furniture for your house, or you could have land, or you could go to University. So I chose University, and I went to McGill to finish up. I had gone to the University of Washington before; I had some credits there, because it was close to Vancouver. Then I went to McGill, and came back to the Vancouver General to teach, because I was really on leave of absence.
And I taught for two years, then I decided I would like to have my Masters. One other nurse was talking about it. So anyway, down I went to Columbia, and I was the first Canadian down there, and I got through my Masters. Well then you have a taste of what you’d want, for your Doctorate. So I was the first nurse with an earned Doctoral degree, brag brag brag. There are many now, over 80, I’m not sure of the numbers.
Director, VGH School of Nursing, with instructor Ruth (Cochrane) Mann, photographed in the 1950s
Director, VGH School of Nursing, with instructor Ruth (Cochrane) Mann, in the 1950s (photo courtesy Sally Thorne, Ph.D., UBC School of Nursing)
George Post: That post war education program that the Canadian government mounted and offered to service people was an incredible thing. The number of people who came back and really launched quite different careers than they might have if they had not had that education available to them.
I think it was absolutely brilliant and outstanding. People would never have gone on for education. Many of the young boys went on, some of them in medical schools, and so on. It was a wonderful program. Education is the answer. It’s certainly the opportunity. That’s so wonderful that they had that program.
George Post: Was McGill University quite crowded in those years when you came back there?
Yes, I can remember sitting on the steps. All universities were I think, but the only place where I could finish my degree and get credits for what I had was at McGill, and I was glad I went there. Oh yes, you were lucky if you got a chair in those days, and you sat on the steps, but that was ok.
McGill University.
McGill Graduate.
George Post: Well you’ve become a world traveller over the course of your life. Was it this original military service that gave you an interest in travel and exploration?
Nurses travelling to Hawaii 1954
Well, I can’t say it was. I know that Lyle Creelman was the Chief Nurse in the World Health Organization, and there were many countries wanting expertise. They wanted somebody desperately to carry out a survey of the Caribbean, the twelve Caribbean schools on the twelve islands, the same way as the one that was carried out in Canada. So I was sent down to do that, I got leave of absence with the CNA. And that led on to another one, then they wanted another one done in Europe, and then another one. The next was Africa, they wanted to set up a West African College of Nurses and get them together. So it all started through the World Health Organization. And the countries at that time would not accept a consultant that didn’t have a PhD or a doctorate, and that is why I got on all these ones. There were very few Canadians. I was the only one at the time. So I really was at the right place at the right time.
George Post: So it didn’t go back to some childhood experience of being keenly interested in geography, or loving maps, or something like that?
No. It was just that they wanted the survey done in the Caribbean the same as it was done (in Canada). And I said, “I don’t know if the CNA will let me go, what will happen”. But they said yes, that I could go down, and I followed up for a couple of years, and that led on. I have done projects in 38 countries. I have just listed them. They were not all surveys, some were different assignments. But there were 38 countries altogether that I visited and worked in. Mostly in nursing education that was my (specialty). Yes, it was great. I’ve been fortunate. Now there aren’t the opportunities, because there are so many more people who are well prepared to go. But then I was the only one that went popping around. And it had its difficulties too, you know, because I’d have the job in Ottawa and then I’d have to come back and pick up where I left off, you know what that’s like.
George Post: You clearly have enjoyed and made a great success of your career in nursing. Was there something that was particularly formative back at the Vancouver hospital, or your service in the military, that tipped you towards a determination to improve nursing, or improve nursing schools? Where did you get this sense of mission about the nursing profession?
Well, when I did this survey of schools of nursing across Canada, I got into that quite by accident too. But that started in 1957, to survey the 25 schools of nursing. I didn’t want to do it, I was on the committee and I said, “No, no, no” I didn’t want to leave home, mother and dad weren’t well and so on…. Eventually you get worn down, and I said yes, I’d try. So that started in 1957, and it ended up in 1960 with the Pilot Project. It was the first survey that had been done of schools of nursing, and the hospitals where they got their training since the Weir Survey, the famous Weir Survey, in 1930. He was an educated scholar and he wrote this great report. I couldn’t do that kind of writing, but I just got to it and we did the survey, we had a committee. They sent me down to the United States to observe how the surveys of schools of nursing were done there, and that was key to my learning about it. I really would not have had the skills nor the vision of how to do it.
George Post: Had you already finished your courses at Columbia at this time? This was after your graduation in ’57?
Let’s see, in ’62 I got my doctorate, and I did these things in between, I didn’t do it all at once. Yes.
George Post: It was coincident with your working on your doctorate.
Yes, right. What I was able to do for my doctorate, because it fits right in to that, is I was so interested in getting started. Once I had finished the survey of the schools of nursing in Canada in February, the meeting wasn’t until June and they had no money to pay me. I didn’t want to go all the way home and have to come back, so I decided I’d go down to Columbia, because I’d been there before for my Master’s. Then I decided in 1960, when they accepted the report, that I’d go back and finish my doctorate. I didn’t have very much money, I knew how to make a choice between buying the book or a good meal, but you do it when you are young and it worked out quite well. So, the one survey then led on to all these other surveys, because people saw them and said, oh, that’s what we want in our country, and so on. It seems strange today in the year 2000, almost 2001, talking about it. But we are now referring to the times when there was very little work going on, very few people that were prepared to do it, or people that had the skills to do it. We learned at University, of course, and at other places. I was just at the right place at the right time I guess.
George Post: But you must also have had a sense that there were changes to be made, or that the system did need to be upgraded and improved.and You’ve obviously absorbed, somewhere along your education and experience, some ability to be dissatisfied with poor standards.
Well, that’s interesting. Have you read that book that just came out called Critical Care by Andre Picard, who writes for the Globe and Mail? Well, he quoted me in there; I said “When I was writing the report of the survey of the schools of nursing across Canada, there were sparks coming out of my pen.” I had no idea that places that called themselves schools of nursing were just, well it was indentured labour, I’ve already used that. They just used the students to staff the hospital with. There was such little regard for their education, and they were housed in some of the poorest of circumstances. Not so in the west, but when you got to the Atlantic provinces and going into some little place in Quebec and so on, it was almost unbelievable. And no one could have done those surveys without being as, furious I guess is the word, as I was. That people would say they were educating nurses, and they were just tossing them on the ward to pick up the education they could. And a good Head Nurse was fined, and so on. Oh, it was very primitive, and I really did write with fire coming out of my pen. I couldn’t believe it. And that report really had an impact, because the documentation was all there, everything we saw was well documented, and we had teams of people in different places. And that did make a change. I always hate to admit it. But I wasn’t alone, it was all the people that worked on those surveys that made the change. And it was really quite dramatic when I look back at it, because we could still be struggling through these miserable hospital schools.
(Laughing) I was persecuted by the Hospital Association because they didn’t want to lose their schools. One, prestige, two, cheap labour. I went to one of their meetings, they’d always invite me to their meetings. And at one meeting they talked about this woman that was going around preaching all this stuff about how terrible the hospital schools were, and she should be put in their place. And oh, they were going on. They didn’t even know I was sitting in the back. But they didn’t like me at all, the hospitals. Some of those administrators, for years after, never forgave me. It wasn’t just me, but I was a good target.
George Post: But that’s the sense of mission that is required for change to be brought about.
Oh, I almost could say I was passionate about it. It was so unbelievable what they were trying… Now, some very good nurses came out of it, but that is because they were good intellectual people, or came from homes where there was a good intellectual atmosphere and so on. But certainly the educational system was poor by any standards and they got away with it. Until this project came up and revealed it all. And it was written in such a simple form; I look back on it now, I really couldn’t have made it simpler. I had my Master’s then, but I am really not a scholarly writer, I can write factually and I can do that reasonably well. But, well, the evidence was so clear. Anyone else could have done it but it just happened that I was selected and I was there. And one thing, I don’t have many strengths but if I have something to do, I put all my energy into getting it done, and then I rest back. Some people can take little rest pauses and so on, but I have to get it done.
At McGill University, in the late 1940’s, an active social life.
Helen’s secondment to the Royal Commission was a stimulating and memorable time for her but she had barely completed writing her final report when she was approached to become Executive Director of the Canadian Nurses Association. With alacrity, she refused to assume that “old maid job”. When negotiations with another candidate failed, Helen was asked to become “acting Executive Director for four months” , until a suitable person could be found. The minutes of the 21-23 of February 1963 meeting state:
(Minutes of the Executive Committee Meeting – 21,22,23 Feb 63)
MOTION
It was moved by the Rev. Sister Decary and seconded by Miss Agnes Maloney
“‘That the President be authorized to name the committee to implement the resolution.”
CARRIED.
LUNCHEON RECESS
The meeting recessed at 12: 30 p.m. for lunch which was served in the Basement Board Room.
AFTERNOON SESSION
OTHER BUSINESS:
Acting Executive Director: The President called the meeting to order at 1:55 p.m. and advised the Executive Committee that Dr. Helen Mussallem, had consented to be the Acting Executive Director, following Miss Stiver’s retirement on April 30, 1963, until the new appointment of Executive Director is made.
I.C.N. Board Meeting: It was announced that the President would be attending the Board Meetings of the International Council of Nurses, in Geneva, in August, 1963. It was unanimously agreed that Dr. Mussallem would accompany Miss MacLennan to the Board Meetings.
Red Cross International Study Centre: The President reported that the Red Cross International Study Centre was being held in Lausanne, Switzerland, August 19-23, 1963. The members of the Executive agreed that Dr. Mussallem should attend the Red Cross International Study Centre which is being held following the I.C.N. Board Meeting.
World Federation of Mental Health: The Executive Committee authorized the President to represent the Canadian Nurses’ Association at the Sixteenth Annual Meeting of the World Federation of Mental Health in Amsterdam, The Netherlands, July 22-26, 1963.
Report of Selections Committee: On the President’s request, Mrs Isobel MacLeod took the chair and the President as Chairman of the Selections Committee presented her report, for the information of the Executive.
It was reported that at the meeting of the Sub-Committee of the Executive Committee on October 18, 1962, the elected Officers were named as a Selections Committee to consider the replacement of the Executive Director. This committee met on October 18 and gave consideration to the names of several persons. The Chairman was authorized to invite letters of application from these persons.
Subsequently, it was felt advisable to publicize the vacancies in national office more widely and an advertisement was placed in The Canadian Nurse Journal and letters were sent to the Executive Secretaries of the Provincial Associations and Directors of University Schools of Nursing.
A roster of names has been compiled and these applications are presently being processed.
The President resumed the chairmanship of the meeting.
DATE AND PLACE OF NEXT MEETING: The next meeting of the Executive Committee, Canadian Nurses’ Association, will be held in Ottawa, Canada, on February 13, 14~ 15, 1964.
ADJOURNMENT: There being no further business, the meeting adjourned at 2:05 p.m. on motion of Miss Claudia Tennant.
29/4/63
Again, Helen requested an extension of her leave of absence from the Vancouver General Hospital and again they complied.
While in Vancouver in late April 1963 to give a keynote address to the Registered Nurses Association of British Columbia annual meeting, Helen went home to Haney for the weekend.
There she saw in the Vancouver Sun (or Province) a large picture of herself announcing her appointment not as “Acting Executive Director” but as Executive Director of CNA. She cried, quietly, “Foul!” On her return to National Office, Helen asked Penny Stiver, the incumbent Executive Director, what had happened. Penny said that she had consulted with Gordon Henderson, CNA’s legal counsel and a highly respected lawyer, nationally and internationally, about Helen’s appointment. Mr. Henderson advised that, as CNA was involved with purchase of land, etc. for a new headquarters, the photo should bear the name of the executive director. So, without consultation, the change was made. Helen understood.
The big day –May 1, 1963 –arrived. With trepidation, Helen sat in the Executive Director’s Chair at 74 Stanley Avenue for the very first time. She felt so alone. Then, the phone rang and it was Laura Barr, Executive Director of the Registered Nurses Association of Ontario. How supportive and how heart-warming! As the day wore on, more and more calls were received –not only from nurse colleagues but from other health organizations, government officials and a large number of nongovernmental organizations.
The die was cast –for four months. All went well until Helen asked the President, Elect MacLennan, to whom she should turn over the Executive Director responsibilities on completion of her term. Electa was so convincing. She asked the Acting Executive Director if she could stay on just until the 1964 biennial meeting in St. John’s, Newfoundland. What a blockbuster meeting that was! CNA outsmarted the Canadian Medical Association by having Mr. Justice Emmett Hall address CNA’s meeting -which just happened to coincide with the CMA meetings. He could have addressed the CMA but he chose CNA. What a coup! Also, Mr. Canada, John Fisher, came to inspire CNA members about Expo 67. Dr. Naegle was there too, addressing the membership on the proposed study of nursing education in Canada. Little did they, and Helen, know that it would be the last time they would see him.
Appointment as Executive Director of the Canadian Nurses Association (5.4.2)
Helen remembers well her trepidation and enthusiasm that first day as Executive Director of CNA. As it was only a four-month appointment, she did not have an orientation or a position description. In those days, there was little emphasis on such frivolities –one just got on with the job.
The fledgling Executive Director had no idea of all that the position entailed but there were a few onerous tasks which loomed on the horizon in addition to the day-to-day “running of National Office”. A search for a suitable site on which to build a CNA National Headquarters was required, and Helen was determined to persuade the President and Executive Committee of the need for a national library resource which she had sorely missed while completing the Pilot Project. She also perceived a very great need for a proper statistical program. There had also been a very strong lobby for the Canadian Nurses Association to host the 1969 Quadrennial Congress of the International Council of Nurses. All of these projects were formidable, of course, but Helen was excited to be getting on with some interesting projects.
CNA had recently undergone a structure study in which the National Office at 74 Stanley Avenue was reorganized. At that time, CNA rented space from the Royal College of Physicians and Surgeons headquarters where it occupied the second floor. Space for staff was reasonably adequate and the Board room was available for CNA use when the College wasn’t using it. This could be quite inconvenient. Another irritant was that there were only two toilets for CNA’s 16-29 female employees. Undaunted, the new Executive Director would use the toilet (forbidden to CNA staff) that was reserved for the College President.
One day, while using the forbidden toilet because she thought the President and everyone else was away, Helen heard three men speaking as they entered the washroom. She was frantic! There she was, seated on the john, trapped! As the men entered, the ever-resourceful Executive Director got off the seat, put her two feet on top of the toilet seat and hung on for dear life. One of the men was Dr. Graham, position, the other, the President and the last was the head of the Finance Committee. As the men performed the necessary functions and were chatting away, Helen thought, “Oh boy, if I make a sound… Dear God, don’t let me slip!” When the three men left, having completed their ablutions, a trembling Helen climbed down off the toilet and never used it again. Sometime later, she told this story to Dr. Graham and he thought it was very funny but, at the time, it was anything but humorous to her.
Alternate unedited version of the preceding story:
There were other humorous, and not so humorous, events that could be recalled. As tenants on the upper floor of the magnificent building owned by the Royal College of Physicians and Surgeons (RCPS) there were certain restrictions imposed. The large office space was completely ours to use as well as the en suite bathroom. But the elegant Board Room had to be booked well in advance for our (CNA) Board meetings. Even then we were not always certain that the College might not have an emergency meeting and we would have the onerous task of rescheduling our meeting. Another area that I was told, on several occasions, was not for our use was the Presidents (RCPS) washroom. As we had only two toilets for our entire female staff I used The Presidents Toilet that was adjacent to my office, always ensuring first that the RCPS President was not in the building. One day I was too busy to look over the railing down to the executive offices to determine if the president was in Ottawa. When seated on the toilet, that was sectioned off in the president’s washroom with partial walls that were opened about 40 cm from the floor up to about 1 1/2 m, I heard three male voices. Yes, they belonged to the president, the general secretary and the executive secretary. What to do: I couldn’t escape without being noticed and by the time I did that, the flies would probably be unzipped. So I crawled up the toilet and put one foot on either side of the toilet and hung on by grasping—with finger tips only—the top of the partial wall. I heard all the noises and conversation and then they left. I climbed down cautiously and dashed back to my office, never to use that toilet again—well almost never. The RCPS Staff were very impressed with my interest in the visit by their president. They thought I was anxious about the extension of the lease and assured me that I was not to worry.
1963
When I was thrust into the post, in May 1963, I had some doubts about my preparation for the position of chief executive officer of a large national organization. My experience as Director of the Vancouver General Hospital School of Nursing; my doctoral studies in the administration of higher education; and my doctoral dissertation had been opportunities to hone my administrative skills but I was apprehensive about my ability to administer such a large, complex enterprise. There was no center, at that time, for additional preparation of CEOs but I believed the principles I had learned during my educational preparation could be applied. This was true to some extent but the role of the CEO was a relatively unknown field in those days.
In 1963, I wrote at the back of my daily calendar:
– A function of management is to establish policies for the control of activities in general and, by way of contrast, to the functions of management, those of the administrator spring from converting policy into practice.
– A good administrator must make the most effective use of existing or available skills.
I found no “existing or available” management skills at CNA headquarters in 1963 so I greeted, with great enthusiasm, the arrival of Lillian Pettigrew on 3 February 1964. She had been Executive Director of the Manitoba Association of Registered Nurses. In our first interview, Lillian told me that one of the great joys of her life was to prepare and finalize the minutes of meetings. Glory halleluiah! There was nothing I could do less well than prepare and write minutes. I was always more interested in action “-in the meetings themselves, the strategy, etc.
And Lillian wrote exquisite minutes.
During my visit with family in Haney, it became obvious that my father’s health was gradually deteriorating. Although he had Parkinson’s Disease his primary health concerns were now related to his abdominal condition. Dad was very proud of my achievements and, especially, of this latest appointment. Fortunately, he was a very successful businessman –and politician –so finances allowed for a permanent practical nurse/housekeeper to help mother meet his health needs. Both were positive and uncomplaining. Occasionally, however, mother was distressed to realize that, after working so hard all their lives, now, when the time had come to enjoy the fruits of their labours, Dad was unable to do so. This visit was the last time I saw Dad alive. I continued to telephone every week (usually Sunday) when possible, and did so on 23 June 1963. Dad was in hospital so the nurse brought him the phone. His voice was clear but weaker.
He told me that my three brothers and two sisters had been in touch with him that day. His last words to me were “Carry on”.
Although I was now CNA Executive Director, I was still required to appear before the Royal Commission on Health Services. My last “interrogation” was scheduled for 24 June 1963 and, although full of grief, I was determined to keep my appointment. I asked Mr. Bleshin, Director of Research, not to tell anyone about Dad’s death as I was afraid I would break down should anyone offer sympathy. The discussions went well and, when they were completed, Mr. Bleshin accompanied me to the elevator. I was too numb to talk. CNA staff were so very supportive.
Georgina Clarke, Director of Administration, had parked her car on Wellington Street so that I could be immediately whisked away to the airport.
Special Projects (Library, Statistics) (5.4.3)
One goal which CNA’s new Executive Director was determined to accomplish was to establish a National Library so Canadian nurses and others would have access to the resources she had so desperately missed while completing the Pilot Project for the Evaluation of Schools of Nursing in Canada. The first task was to find a suitable Librarian. The Executive Committee gave permission for CNA to hire a part-time Librarian and Helen interviewed all of the applicants. One person –Margaret Parkin –stood out above all the rest. Margaret, however, wanted a full-time position with a specialty library. As it turned out, she was the most suitable candidate for the position and was eventually hired.
When Margaret Parkin came to National Office at 74 Stanley Avenue, CNA’s Library was a pile of 350 outdated books stacked in the corner. Together, Margaret and Helen established a library that today serves not only nurses but the whole health community and others from all across Canada.
Helen’s second self-appointed task was to find a person qualified to establish a statistical program. She was very fortunate to recruit Lois Graham Cumming who had married a Canadian and had recently relocated from Washington, D.C. where she had been with NIH. Lois developed a tremendous statistical program which was the envy of other associations and was used extensively by governments and others.
Helen recalls many humorous events which took place at 74 Stanley. She remembers, vividly, two visiting nurses from Africa who had come to CNA as part of a world-wide tour. On the day of their visit, it was Ramadan and, of course, they were not allowed to eat between sunrise and sundown. The older nurse was obviously very devoted and went on talking with Helen all morning and until noon and past. Sandwiches, which were made by the superintendent’s wife, were delivered but she didn’t eat. The younger visitor finally asked Helen if she could speak with her in the washroom. She said, “I am so hungry. Don’t tell my friend but I would like to have something to eat.” Helen brought her some sandwiches which she ate in the toilet. That evening, CNA’s Executive Director invited the international visitors to dinner at the Chateau Laurier Grill which was one of the best dining places in all of Ottawa. It was a glorious meal with a huge hind of beef served on a gorgeous silver tray with a great silver cover on it. Both ladies ordered the roast beef. The famished senior nurse quickly polished off her dinner and then said she would like to have another piece of beef. Helen informed the waiter. The waiter called the head waiter who asked Helen to speak with him away from the table. Apologetically, he advised that if the lady had another piece of beef, he would have to charge her for two meals. “Well, go ahead,” said Helen. So, CNA’s African visitor made up for the meal she missed between sunrise and sundown and was probably surprised that her companion was satisfied with the meal that had been served to them.
Then there were the visits of Ottawa Mayor, Dr. Charlotte Whitton. The first time she came to my office, she simply barged in. No appointment — no nothing. She plunked herself down in the chair opposite mine and inexplicably said, “I bet Queen Victoria wouldn’t know what to do with a pregnant soldier.” I hardly had time to turn this sentence around in my mind before she told me she was producing a film of interviews with “prominent Ottawa women” and I was to be one.
Enough said — I was interviewed. It was a long, time-consuming assignment. Dr. Whitton always called me at 6:30 P.M., often when I was preparing dinner for guests. One never said “no” or “I’m too busy now” to Charlotte Whitton. Our conversations would take up to half an hour so I learned to put the phone on the kitchen counter and say into the receiver from time to time, “very interesting Dr. Whitton”. I eventually learned that her comment about Queen Victoria referred to the her significant role in arranging for assistance for women in the armed services, from overseas or in other locations across Canada, who became pregnant out of wedlock and required rehabilitation.
Throughout the period 1 May 1963 to 1 April 1966, I was fortunate to lead a very hard-working and supportive staff — two of whom at the time of writing (1995) are still valued CNA staff members, namely, Pat Mohr and Pierrette Hotte. Both have advanced to senior positions and their supervisor, Beryl Darling still maintains contact. Others who contributed, significantly, were Lillian Pettigrew (now deceased) who was Associate Executive Director; June (Ferguson) Graeme Fraser who was Public Relations Officer; Georgina Clarke (now deceased) who was Office Manager, and Mr. Ernest Van Raalte, who conducted the Stevenson-Kellogg study on the structure of CNA and later became General Manager. His structural plan was approved by the Executive Committee but was never readily understood by me. Its main purpose was to integrate the staff of The Canadian Nurse/L’infirmiere canadienne with CNA staff. The integration was successful but I found that having professional staff report to me through a non-nurse was not workable. Many modifications were made and approved by the Executive Committee. Already mentioned were two senior staff members who made a significant impact on Canadian nursing, namely, Margaret Parkin, Librarian and Lois Graham-Cumming, Statistician. Although I had authority to hire only a part-time Librarian, when M. Parkin came along and would work only full-time, her expertise was essential to develop the kind of library I had envisioned so I brought her on staff and my decision was not questioned -especially when her sterling qualities became known to the Executive Committee.
These were some of the staff at the 74 Stanley Avenue location but, in the beginning of my tenure at CNA, both professional and support staff were very small in number.
First International Initiatives 1963 (5.4.5)
My first, major responsibility as CNA Executive Director was to attend two international meetings. I had hardly warmed the seat of my chair when I accompanied the CNA President to the Grand Council Meetings of International Council of Nurses (now Council of National Representatives -CNR) held in Geneva, Switzerland in 1963. I remember well the tiny room in John Mott House where representatives met. John Mott House is located just a few meters from ICN’s present headquarters at 3, place Jean-Marteau (rue de l’ancien port). One of the most controversial subjects at that, my first ICN meeting, was related to the move of ICN headquarters from London to Geneva. Much emotion was attached to this issue as ICN began in the U.K. where great leadership had been provided in ICN’s initial and formative years and, indeed, up to 1963. Other items of interest to me were the ICN program relating to nursing education and nursing service. I was fascinated to hear the comments of member presidents from far away countries in Africa, South America, India, the Middle East, etc. This was the very first time I had ever been in a room with so many international nurses and I was excited and intimidated. Little did I know, at that time, what the future held for me. The financial reports were also intriguing as we tried to work with both British Pounds and Swiss Francs. The move of ICN staff to Geneva was also cause for tension. Pence and francs were carefully guarded. My main role was to advise the CNA President, Electa MacLennan, but I did speak up when I had something to add to the debate. At that meeting I also learned of the high regard with which the Canadian delegation was held, due in no small measure to the reputation of Lester B. Pearson.
Immediately following the ICN session in Geneva, I attended meetings of the International Red Cross Society in Lausanne, Switzerland, This time, I was on my own, representing Canada with a senior member of the Canadian Red Cross, Helen MacArthur. Helen was well known in international circles and was very highly respected. Once again, I was thrilled with the international milieu. Discussions were fascinating and touched on all aspects of the work of the International Committee of Red Cross Societies and the Red Crescent. I was much impressed with the discussions on the Rights of Nurses under the Geneva Convention as I had little knowledge then of the many critical situations facing nurses at that time.
As always, then and now, there were a number of elaborate receptions. I recall one that was hosted by the head of the Canton of Viau. He spoke with me in French and uncertain English, and I responded in English and uncertain French. He insisted on driving me, and three others, to our hotels. He dropped the other three off, one by one, and, in doing so, passed my hotel twice. Each time, I said “Chez moi,” but he kept driving. When my colleagues had all left, he parked the car and my worst fears became a reality. Now, how does one handle this situation without creating an international incident? We had a real tussle but he eventually gave up and, as he drove me back to my hotel, he said three times, “You are a wet blankette”.
Despite his lack of fluent English, he managed to convey his summary of me very well!
Instead of returning directly to Ottawa, my staff persuaded me to “take a week off” as I had been working a seven-day week of mostly ten to twelve hour days. I chose to go to Paris and then on to London. All was arranged by Cooks Tours.
I saw everything a tourist should see in Paris –Le Louvre (so disappointed with the Mona Lisa; I liked Winged Victory much better); VersaiIle, the Eiffel Tower, the Left Bank, the magnificent cathedrals, Place Pigalle (wow!) etc.
One of my main objectives in Paris was to follow the advice of my hairdresser at Friemans Antoinne Salon in Ottawa and visit the world’s master hairdresser, Antoine, at 3, rue Cambon, in Paris to buy a really superior wig. We wore them often in those days … real wigs made from real hair. I used wigs, complete with hat box, when travelling during the Pilot Project for the Evaluation of Schools of Nursing. What an experience! I arrived at Antoine’s at 09:00 and sat in a posh area awaiting THE MASTER. Around 10:00, a tall, fashionably-dressed man, with painted fingernails and outlandish shoes, breezed in followed by an entourage of young men who adoringly watched his every move. He passed the glass coffin (readied, I was told, for the Great Man Himself) and went to the etageres returning with three wigs. Without saying a word, he came to where I was seated, passed his painted fingernails through my hair –and said something like “ugh”. He then flourished each wig next to my hair, as the spellbound young men looked on, until He finally decided on one of the three. He asked that I be “preparer” for the transformation. My own hair was washed and dried with the entourage looking on. Then THE WIG was put on and curled on my head!?! I, and my wig, sat under the dryer and, when the appropriate time came, I was pulled out. All the while, I wondered how much all of this would cost as I had a limited amount of money with me and no credit card. Well, when I emerged from under the dryer, complete with wig, I must admit it all looked good –very good. Delicately, I asked for “l’addition” –$300 U.S. That was like $1,000 Canadian today and, luckily, I had exactly $300 left in traveller’s cheques. I departed. No receipts. No nothing. Not at Chez Antoinne!
On arrival at Heathrow Airport in London, I looked for a uniformed Cook’s representative as I had in Paris where he had spotted me right away. In London, however, I looked around and, as no representative approached me, I picked up my luggage and headed off to hail a cab. Noticing a man in a Cook’s uniform, I casually asked if he knew who had been sent to meet Dr. Mussallem. Startled, he responded, “It’s me!” When I told him I was Dr. Mussallem, Executive Director of CNA, he apologized and said he had been looking for someone who fit the picture of an Executive Director of a women’s organization –someone “much older”. He had seen me deplane but was sure this chic young lady in mauve chiffon and beautifully coifed hair was not his person. What wonders Antoine had worked in Paris! My driver escorted me by Cook’s private limousine to the elegant Mayfair Hotel and “the nightingales sang in Berkley Square”. He told me that his evening was free and he would be delighted to take me out “privately”, i.e., at his own expense. Amused, I said I was very tired after Paris (I wasn’t) but perhaps another time. He gave me all the coupons and mounds of material for my London stay –and departed.
As I thought I might not see London again (my first visit had been during WWII when all the guards were in khaki), I saw all the usual tourist sites and was impressed with the reconstruction since the bombings I had witnessed during the war. One humorous incident took place on my last “free” day in London. It was a grey, drizzly day and, as I had planned to go to ICN’s headquarters on Dean Tench Street, I thought I should wear some sort of protection for my shoes so I would not soil the carpets. I had seen pictures of the entrance hall of ICN’s London headquarters and I didn’t think mud would look too good on those antique carpets. On Regent Street, I spotted two middle-aged ladies waiting for a bus and asked them, very politely and innocently, where I might buy some rubbers. Dressed in my raincoat, I followed their directions and walked three blocks down, turned left and found a chemist’s shop. It was not until I got there that it dawned on me that the ladies had misunderstood what I meant when I asked for rubbers. Even though we speak the same language in both countries, there are flaws in our communication.
On my return to Canada and CNA, there was a great accumulation of correspondence awaiting attention, documents requiring study and action, many articles to be read, and decisions to be made. Staff members with problems required immediate appointments, reports had to be written for the Executive Committee, meetings of external committees must be attended, and some social functions required my attendance. In short, there was what was to become the usual post-field trip, back-breaking workload to deal with.
The dust had scarcely settled when I received a call from Lyle Creelman, Chief Nurse at the World Health Organization, asking me to attend a WHO Scientific Meeting on Research in Nursing. She made it quite clear that this was a highly-prestigious meeting attended by only a few select experts, worldwide. As this was a WHO Scientific Group on Health, three especially-qualified public health doctors must attend and, as it involved nursing and research, there would also be three nurse experts in research in attendance. I was asked to be the member from the Americas. The public health physicians were selected from the U.K., the Middle East and Greece. I remember so fondly my flight to Geneva. It was first class all the way, such a contrast from flying “steerage” on the old North Star planes. That meeting, convened at WHO Headquarters in Geneva, remains in my memory one of those extra special events. We gathered the first morning to find one of our delegates, Dr. Ewing from the U.K., missing. Dr. Candau, WHO Director-General, greeted us at that initial meeting and asked that a chairman be elected. After his greeting and a general outline of the goals of the meeting, he called for nominations and the election of a Chair. First thing I knew, my name was proposed and I was asked if I would accept the Chair. Modestly I responded, “Yes, if I am elected.” He replied, “You have just been elected. Please take the Chair.” What I didn’t know then was that all of this had been arranged ahead of time. After I mumbled a few words, Lyle Creelman advised that we should wait for the U.K. representative to join us so I called for adjournment. This gave me an opportunity to review the agenda and to determine what my responsibilities would be during the week’s session. We reconvened about 11:00, with Dr. Ewing present, and I made a few introductory remarks. Dr. Ewing then asked for the floor, and floored us by advising that he was late because he failed to see the reason for the meeting. “Surely,” he remarked, “you don’t think nurses do research. Nursing is not a pure science.” Flabbergasted, we tried to remain calm and provide him with a rational explanation, i.e., that nursing was an applied science and, indeed, was a subject for research. He just sat there, in a state of gloom. When we recessed for lunch, I rushed over to the smartest and cutest member of the group and told her that she must invite Dr. Ewing to lunch and enlighten him on nursing research. He was more compliant after lunch, and my co-conspirator later told me he had been resistant but listened well.
The WHO meetings were intense, with much heated debate. I recall, during one discussion, Dr. Vellorous of Greece came forth with what I thought was a good point. As Chairman, I asked “Dr. Vellorous, would you like to throw out that idea?” “No, Madam Chair,” he said “I want to throw it in.”
In addition to the lengthy and exhausting sessions, each day we had to check the report being written by the rapporteurs for accuracy, style, etc. It was a trying job but, eventually, by Saturday morning, we had concluded the meetings and a rough draft of the report had been written. As a reward for all of this sustained labour, we were invited to spend the weekend at Lyle Creelman’s chalet at Champery, in nearby France. What a glorious time we had with Lyle and Margaret Scott-Wright. We did have some difficulty in getting to the chalet, however, as part of the road was washed out and we had to crawl along on logs with our supplies strapped to our backs. When I arrived at the end of the log, Lyle was hysterical with laughter. She said she couldn’t believe that the First Scientific Group on Nursing Research had fallen to the level of crawling on logs across deep ravines –such a contrast to our lofty and proper posture at the WHO meetings in Geneva!
The return trip to Ottawa was on Swiss Air, First Class. Life doesn’t get much better. As soon as we reached cruising altitude, the steward came to me with a silver tray loaded with Iranian caviar and champagne. I, of course, immediately looked at my watch but he reassured me that it was proper to drink at that hour as, in the air, time didn’t count. That was my first real taste of caviar and I have loved it ever since!
CNA Initiatives (5.4.6)
My first two international assignments (ICN-Geneva and Red CrossLausanne) gave me a peek into the expansive, wonderful and intriguing world of health at the national and international level. When I returned to Ottawa and National Office internal and external work seemed to be progressing reasonably well, I reminded the CNA President that my four month commitment to CNA was nearing an end. She assured me that the Executive Committee was searching for a replacement but would I consider staying, just until the June 1964 biennial meeting. There was still much work to be done following our presentation of briefs (in 1963) to the Special Committee on Aging, the Royal Commission on Bilingualism and Biculturalism and the Canadian Conference on Mental Retardation. As I was able to get an extension of my leave of absence from Vancouver General Hospital, I agreed. Little did I know then that there were many exciting projects coming up and that I might soon have an Associate Executive Director to share the increasingly-heavy burdens of my office.
A whole new world opened for me in 1964. CNA seemed to plunge into high gear. Among the activities which stimulated CNA and its staff were:
– Three projects arising from the recommendations of the PPESN were getting underway: The School Improvement Program being directed by Glenna Rowsell; The Evaluation of Quality being directed by Lillian Campion; and the Study of Nursing Education headed by Kaspar Naegle.
– Initiation of the statistical program, involving all provincial associations in the collection of data on the total nurse population in Canada. (Prior to this, the only statistics available were the number of nurses who belonged to their provincial nurses’ association.)
– Reactivation of the Nursing Research Index. Initial work on this project revealed that there were over 100 known studies on nursing in Canada. These were collected and listed in a card index.
– The CNA/CMA/CHA Liaison Committee agreed that, whenever possible, a tripartite approach should be made to the federal government.
– CNA established a Standing Committee on Social and Economic Welfare. Its establishment was fraught with opposition from those provincial associations which strongly believed that collective bargaining was “not professional”. They were deeply concerned that nurses might even contemplate “going on strike”.
– A very active National Office Auxiliary kept me busy in an effort to find suitable tasks for them. They were a sincere, knowledgeable group but I was unsuccessful in setting up a meaningful program.
– An unofficial communication from the National League tor Nursing (NLN) in the U.S. conveyed the serious news that the NLN was considering the withdrawal of NLN exams in jurisdictions outside the U.S. An ad hoc committee was appointed to look at ways and means of solving this problem. Perhaps six provincial associations were using the exams for students seeking registration in their province.
– Legal matters relating to the use, by White Sister Uniform Company, of the new CNA logo — the leaf and the lamp – on their uniforms.
– CNA was asked to participate in Expo ’67.
– My doctoral dissertation was published with the title Development of Nursing Education Programs Within the General Educational System of Canada. It sold for $3.00 each and was reprinted twice.
– A strategy was developed to propose Alice Girard as President of ICN. I sent letters, requesting support for the nomination of Alice Girard, to 58 ICN member countries. (At the 1965 Quadrennial Congress, she was elected by acclamation.)
On invitation, Alice Smith and I worked very hard to develop a Centennial Project. The plan was to have nurses from the southern belt of Canada exchange positions with northern nurses for a two-week period so more nurses might be attracted to “north of 60”, where they were really needed. Alice developed an exquisite plan and presented it to the Board, using suitable visual aids. The Board raised all sorts of obstacles, and our inspired project, which we called “Northern Lamp”, was snuffed out.
CNA 1964 Annual General Meeting St Johns Newfoundland
Joint Committee of CNA/CMA/CHA
As Director of Special Studies, I soon realized that there were of number of “external” boards or committees on which I sat by virtue of my position as CNA Executive Director. Two of these ‘Joint” boards were the Nursing Unit Administration program (CNA and CHA) and the CMA/CNA/CHA Committee on Nursing. In 1964, at the request of CNA, the CMA/CNA/CHA Committee on Nursing changed its name to the Joint Committee of CMA/CNA/CHA to reflect a change in focus and to facilitate discussion on matters relating to all three organizations, rather than on problems which dealt only with nursing.
The Nursing Unit Administration (NUA) program was unique in North America as it was sponsored by two national, voluntary organizations. It began, prior to my tenure as Executive Director, in response to a recognized need to upgrade the management skills of nurse managers (head nurses) in acute care hospitals. When I became Executive Director, the course was still in its formative stage but, due to the expertise and skill of the director of the program, Kathleen Ruane, the program progressed “on course” and was meeting its objectives. When I attended my first NUA meeting, I detected tension between CHA and CNA representatives. CHA members believed that they should have sole authority in setting the direction for the course since it was directed at head nurses in “their hospitals”. This was a futile posture, however, since the Kellogg grant which initially founded the program had been adamant that CNA should be an equal partner in the program.
The CMA/CNA/CHA Joint Committee on Nursing, renamed the Liaison Committee of CMA/CNA/CHA, was, to some extent, a revelation of the emerging importance of CNA in the tripartite world of health. CNA had equal, joint, permanent representation with CHA and CMA on this committee.
I remember well my first meeting with this tripartite group. The entire agenda was compiled of a list of problems in nursing which the other two organizations were going to solve. I should state, parenthetically, that this committee first came into being during periods in WWII when there was a severe shortage of nurses in hospitals and the medical and hospital associations discussed this problem at great length, with questionable success. When I became CNA Executive Director, I became aware of the joint committee discussions through minutes of meetings and other documents. I was, however, shocked to find that CNA was being placed in the position of accepting advice from CMA and CHA as to action it should take in relation to nursing’s problems but that CNA’s advice on the problems facing medicine and hospitals was neither sought nor wanted. Without previous discussion with my president, Electa MacLennan, I innocently — and boldly — asked why the problems of medicine and hospitals were not being discussed at the meeting as well. Dr. Young, the external chair of the committee, replied that those problems could be discussed at the next meeting. I became concerned that I might have caused a disruption of the committee which might have serious consequences. At our next meeting, CHA representatives appeared at the appointed time but CMA members were absent. About 15 minutes late, in they marched — in single file, and sat down. Before the meeting could be called to order, CMA stated its position: they were unwilling to have any discussion of CMA concerns brought to the meeting. They would withdraw first! After somewhat cordial, if tense, discussion of agenda items, the CMA President, Dr. Frank Turnbull, said that he did not know the real value of the committee other than it provided an opportunity, twice yearly, for the presidents and executive directors of the three organizations to sit across the table and have a good, free-flowing discussion. This, he believed, was worthwhile. The day and the committee was saved. Subsequent, recorded actions of this committee suggest that Dr. Turnbull was right.
My relationship with the Canadian Nurses Foundation (CNF) was interesting and varied from great hope to despair as to its future and its goal of providing selected nurses with the opportunity to pursue graduate education. My commitment and dedication to this goal was another spin-off from my cross-Canada surveys of nursing education in both hospital and university schools of nursing. I knew that, if nursing service was to improve, the education of nurses for that service must, likewise, be improved. Along with many other “senior” nurses, I recognized that advanced education for nurses was imperative if nurses were to be accepted as an equal voice in the decision-making circles of the health care system. A personal note adds validity to this statement. As CNA’s Director of Special Studies (1960-63) I attended the CMA CHA CNA Committee meetings to report on the status of nursing education in Canada and to describe to the committee the projects undertaken by CNA which had been initiated as a result of the recommendations of my Pilot Project on the Evaluation of Schools of Nursing. The first meeting I attended was held at CMA headquarters in Toronto. The group from CNA entered the committee room through the side door. All other representatives seemed to come from somewhere else. At the next meeting, after I obtained my doctorate in 1962, I was met at the front door by the CMA General Secretary. I was astounded to be ushered in, to walk on the richly-carpeted hallway, and to be told that the CMA president would like to see me. Three times I was referred to as DOCTOR Mussallem. Then, I was taken to the committee room at the rear of the building. I was suspicious that my doctorate (the first earned by a nurse in Canada) might have been responsible for this unusual gesture and the CNA Executive Director, Penny Stiver, confirmed my suspicion.
In 1961, while I was Director of Special Studies, the CNA Executive Committee -influenced, perhaps, by the findings of the Pilot Project for Evaluation of Schools of Nursing –decided that “… the time had come when the Canadian Nurses Association should consider establishing a foundation”. A Special Committee, called the Canadian Nurses Association Foundation, was created in 1961 to work out the details necessary to establish such a foundation.
In February 1962, the Special Committee, Canadian Nurses’ Association Foundation, presented its report. The Executive Committee decided at this meeting that the Foundation would be known as the Canadian Nurses Foundation (CNF), and that its purposes would be: to provide financial support in the form of awards to nurses pursuing graduate studies at the masters and doctoral levels; to provide grants for nursing research; and to administer funds donated to the Foundation for the above purposes. CNF came into being in 1962 when the Kellogg Foundation awarded CNA a donation of $150,000 (U.S.). The preparation of the brief for the Kellogg Foundation requesting $150,000 (U.S.) for the establishment of CNF (and the accompanying strategies) and CNA’s success in obtaining these funds – to be spread over a five year period –was due primarily to the expert and scholarly work of Katherine MacLaggan. The CNA Executive Committee was preparing to have this Foundation set up within CNA but as the Kellogg Foundation required a receipt from a “charitable” agency for income tax purposes, a foundation was created by CNA to facilitate this request. In the early years of the Foundation, office space and administrative services were provided by CNA.
When the Kellogg grant arrived in Ottawa, CNF was advised that the amount allocated for 1962 scholarships must be awarded before the end of August 1962. Word of the new scholarships was disseminated and a number of applications were received at CNA headquarters. Then, I gather, a Selections Committee needed to be appointed. As it was early August, few staff or other suitable persons were available. I had just successfully defended my doctoral dissertation at Columbia and had returned to Ottawa, as promised. On arrival, I was advised that I was to work with Katherine MacLaggan to select the first “scholars”.
At the appointed time, I met with Katherine in her room at the Chateau Laurier. We worked very hard to develop criteria and to assess each application. A decision had to be made. Should all applications be ranked and scholarships awarded to only the top few, or should we ensure that each application was “worthy of an award” and spread the money over the qualified candidates? After assuring ourselves that each candidate merited an award, we chose the latter option. Two applications were rejected due to incomplete documentation. All the monies for 1962 were disseminated and, in retrospect, I believe we did an exceptional job.
In May of 1963, when I became CNA Executive Director, I inherited the responsibility for the administration of CNF. The monies from Kellogg were well used on fellowship and scholarship awards as, initially, CNA bore the entire administrative costs. However, the CNF Board, composed of half CNF members and half CNA members, had great ideas about CNF’s potential as a free-standing organization without CNA connections or controls. The CNF Board was appointed, and the part-time Executive Director (Lois Graham-Cumming) designated a member in each province as a CNF representative. The provincial associations were by-passed and, indeed, CNF attempted to set up an organization as “strong and powerful” as CNA. They would be free to solicit large sums of money for CNF and not “be hampered” by CNA. This “completely separate” organization did not survive for long and, in 1966, CNF became more closely allied with CNA while maintaining its separate identity as required by the Letters Patent. I later became Executive Secretary/Treasurer of CNF.
One of CNF’s perennial problems was always to find sufficient funds to maintain the scholarship program. The need was very great and hardly any other monies were available for nursing students studying at the masters or doctoral level. When the Kellogg money ran out, great efforts were made to obtain more funds but results were dismal. Each Selections Committee was faced with the problem of making awards with shrinking budgeted funds. One year, in the early 70s, when Glennis Zilm, Assistant Editor, was writing an article for The Canadian Nurse, she asked me what would be done at the next Selections Committee as funds were so low. I said, “Let’s go for broke!” She published my remark and, due to the efforts of provincial associations (some gave a yearly donation based on membership), the funds grew and then stabilized. It was a real roller coaster ride and I spent many of my precious “extra hours” doing CNF work. Often, I was asked why I worked so hard for CNF. My answer was honest and simple. When I studied for my masters and doctoral degrees with a very small income –having to decide between buying a book or eating dinner –I became dedicated to doing what I could, in my lifetime, to prevent others from facing similar circumstances.